
Also, scientists stand apart from their subject matter--as distantly as possible. Physicians, on the contrary, are in "a relationship" with patients. 2/
Sorry, Dr. Jha, but you shouldn't confuse medical care with the scientific enterprise. Although the 2 are commonly conflated, they are really distinct. 1/
The hearings are meant as a questioning of the scientific process
— Ashish K. Jha, MD, MPH (@ashishkjha) December 7, 2020
To sew doubt on what we know and how we know it
So a group of us organized a response, which we just posted on our website
It isn't pro or anti hydroxy
Its about the scientific method and why it matters
2/3
Also, scientists stand apart from their subject matter--as distantly as possible. Physicians, on the contrary, are in "a relationship" with patients. 2/
First, scientific knowledge is often limited or provisional, especially with a new disease.
Second, for every patient there are myriad circumstances that influence a medical decision. /3
Fourth--and most pertinent here--one cannot narrowly limit the scientific knowledge to only RCTs as you do in your statement. /4
I won't rehash all the arguments here (and there are many!) but I'm sure you're familiar with this piece by Dr. Frieden from only a couple of years ago https://t.co/f7jHvDujUZ /5
My point is that your attacks miss the point: Medical standards cannot be reduced to scientific ones. /12
If you have an interest in the historical background for this, here are a couple of the pieces that I wrote on this topic a few years ago: /14
https://t.co/q5ECfaN47b
More from Science




1. I find it remarkable that some medics and scientists aren’t raising their voices to make children as safe as possible. The comment about children being less infectious than adults is unsupported by evidence.
2. @c_drosten has talked about this extensively and @dgurdasani1 and @DrZoeHyde have repeatedly pointed out flaws in the studies which have purported to show this. Now for the other assertion: children are very rarely ill with COVID19.
3. Children seem to suffer less with acute illness, but we have no idea of the long-term impact of infection. We do know #LongCovid affects some children. @LongCovidKids now speaks for 1,500 children struggling with a wide range of long-term symptoms.
4. 1,500 children whose parents found a small campaign group. How many more are out there? We don’t know. ONS data suggests there might be many, but the issue hasn’t been studied sufficiently well or long enough for a definitive answer.
5. Some people have talked about #COVID19 being this generation’s Polio. According to US CDC, Polio resulted in inapparent infection in more than 99% of people. Severe disease occurred in a tiny fraction of those infected. Source:
I find it remarkable that a section of society not rejoicing that children very rarely ill with COVID compared to other viruses and much less infectious than adults
— Michael Absoud \U0001f499 (@MAbsoud) February 12, 2021
Instead trying prove the opposite!
Why??
2. @c_drosten has talked about this extensively and @dgurdasani1 and @DrZoeHyde have repeatedly pointed out flaws in the studies which have purported to show this. Now for the other assertion: children are very rarely ill with COVID19.
3. Children seem to suffer less with acute illness, but we have no idea of the long-term impact of infection. We do know #LongCovid affects some children. @LongCovidKids now speaks for 1,500 children struggling with a wide range of long-term symptoms.
4. 1,500 children whose parents found a small campaign group. How many more are out there? We don’t know. ONS data suggests there might be many, but the issue hasn’t been studied sufficiently well or long enough for a definitive answer.
5. Some people have talked about #COVID19 being this generation’s Polio. According to US CDC, Polio resulted in inapparent infection in more than 99% of people. Severe disease occurred in a tiny fraction of those infected. Source:

Ever since @JesseJenkins and colleagues work on a zero carbon US and this work by @DrChrisClack and colleagues on incorporating DER, I've been having the following set of thoughts about how to reduce the risk of failure in a US clean energy buildout. Bottom line is much more DER.
Typically, when we see zero-carbon electricity coupled to electrification of transport and buildings, implicitly standing behind that is totally unprecedented buildout of the transmission system. The team from Princeton's modeling work has this in spades for example.
But that, more even than the new generation required, runs straight into a thicket/woodchipper of environmental laws and public objections that currently (and for the last 50y) limit new transmission in the US. We built most transmission prior to the advent of environmental law.
So what these studies are really (implicitly) saying is that NEPA, CEQA, ESA, §404 permitting, eminent domain law, etc, - and the public and democratic objections that drive them - will have to change in order to accommodate the necessary transmission buildout.
I live in a D supermajority state that has, for at least the last 20 years, been in the midst of a housing crisis that creates punishing impacts for people's lives in the here-and-now and is arguably mostly caused by the same issues that create the transmission bottlenecks.
Rooftop solar can play a key role in a transition to 100% renewable energy - and it can help American's pocketbooks #GoSolarhttps://t.co/6p9jb62EGW
— Environment America (@EnvAm) January 14, 2021
Typically, when we see zero-carbon electricity coupled to electrification of transport and buildings, implicitly standing behind that is totally unprecedented buildout of the transmission system. The team from Princeton's modeling work has this in spades for example.
But that, more even than the new generation required, runs straight into a thicket/woodchipper of environmental laws and public objections that currently (and for the last 50y) limit new transmission in the US. We built most transmission prior to the advent of environmental law.
So what these studies are really (implicitly) saying is that NEPA, CEQA, ESA, §404 permitting, eminent domain law, etc, - and the public and democratic objections that drive them - will have to change in order to accommodate the necessary transmission buildout.
I live in a D supermajority state that has, for at least the last 20 years, been in the midst of a housing crisis that creates punishing impacts for people's lives in the here-and-now and is arguably mostly caused by the same issues that create the transmission bottlenecks.



You May Also Like









So friends here is the thread on the recommended pathway for new entrants in the stock market.
Here I will share what I believe are essentials for anybody who is interested in stock markets and the resources to learn them, its from my experience and by no means exhaustive..
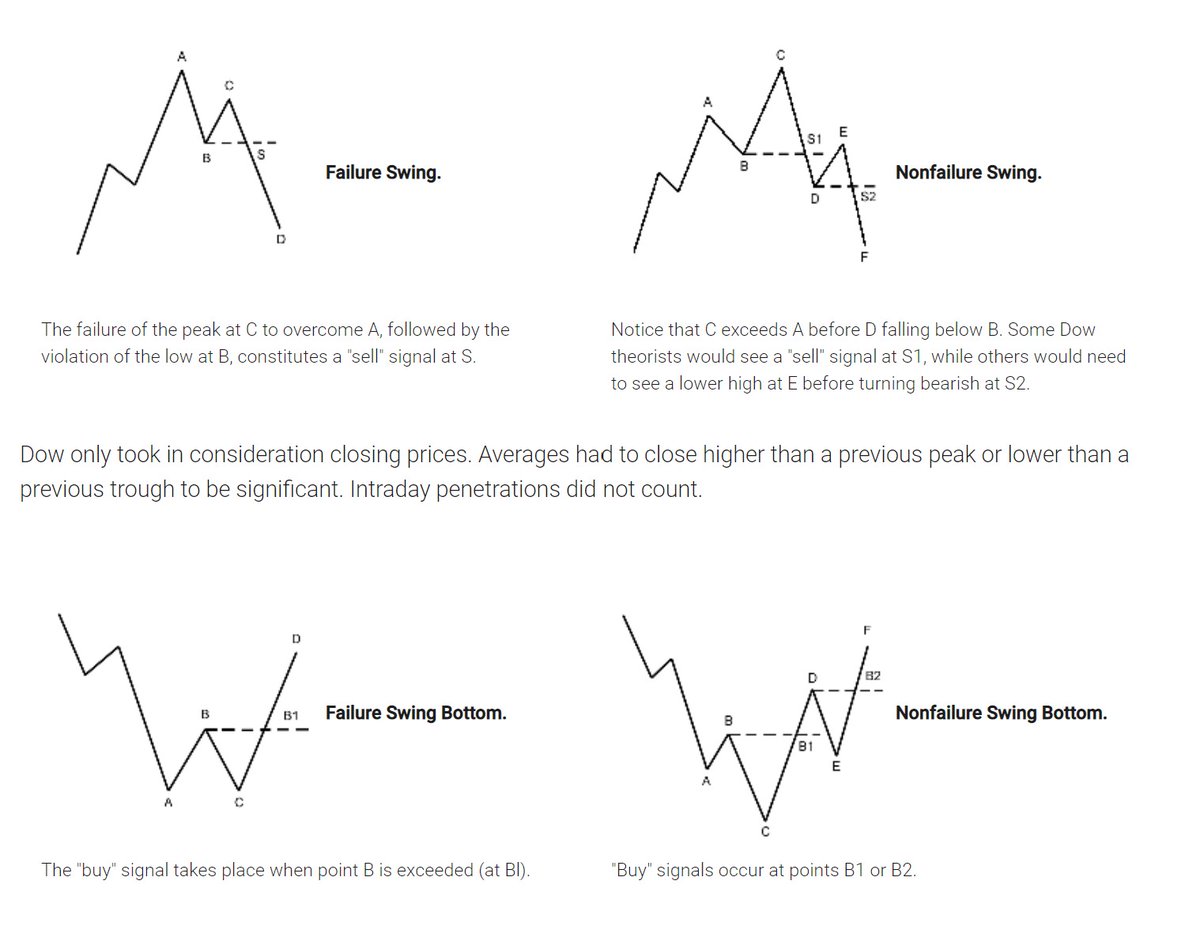
First the very basic : The Dow theory, Everybody must have basic understanding of it and must learn to observe High Highs, Higher Lows, Lower Highs and Lowers lows on charts and their
Even those who are more inclined towards fundamental side can also benefit from Dow theory, as it can hint start & end of Bull/Bear runs thereby indication entry and exits.
Next basic is Wyckoff's Theory. It tells how accumulation and distribution happens with regularity and how the market actually
Dow theory is old but
Here I will share what I believe are essentials for anybody who is interested in stock markets and the resources to learn them, its from my experience and by no means exhaustive..
First the very basic : The Dow theory, Everybody must have basic understanding of it and must learn to observe High Highs, Higher Lows, Lower Highs and Lowers lows on charts and their
Even those who are more inclined towards fundamental side can also benefit from Dow theory, as it can hint start & end of Bull/Bear runs thereby indication entry and exits.
Next basic is Wyckoff's Theory. It tells how accumulation and distribution happens with regularity and how the market actually
Dow theory is old but
Old is Gold....
— Professor (@DillikiBiili) January 23, 2020
this Bharti Airtel chart is a true copy of the Wyckoff Pattern propounded in 1931....... pic.twitter.com/tQ1PNebq7d