
It's 2021! Time for a crash course in four terms that I often see mixed up when people talk about testing: sensitivity, specificity, positive predictive value, negative predictive value.
These terms help us talk about how accurate a test is, but from different viewpoints. 1/
A test that is very *specific* will be very good at accurately ruling out infection in people who are not infected. 3/
Of the 10 people infected, 8 test + (true +), 2 test - (false -).
Of the 90 people uninfected, 89 test - (true -), 1 tests + (false +). 7/
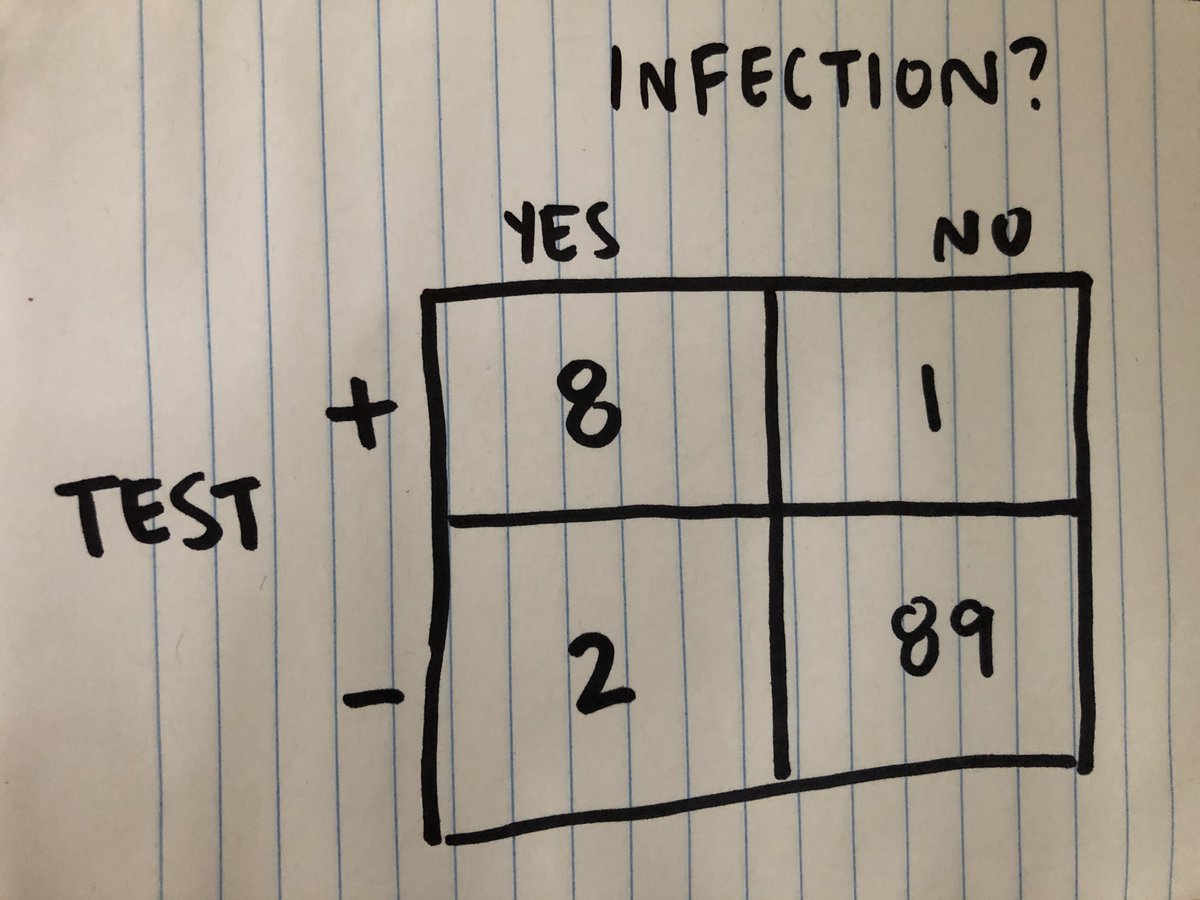
The test's positive predictive value is true positives/(true positives + false positives): 8/9, or 88.9%. It's the proportion of positives, out of all the positives, that were accurate. 10/

More from Education

Trending news of The Rock's daughter Simone Johnson's announcing her new Stage Name is breaking our Versus tool because "Wrestling Name" isn't in our database!
Here's the most useful #Factualist comparison pages #Thread 🧵

What is the difference between “pseudonym” and “stage name?”
Pseudonym means “a fictitious name (more literally, a false name), as those used by writers and movie stars,” while stage name is “the pseudonym of an entertainer.”
https://t.co/hT5XPkTepy #english #wiki #wikidiff
People also found this comparison helpful:
Alias #versus Stage Name: What’s the difference?
Alias means “another name; an assumed name,” while stage name means “the pseudonym of an entertainer.”
https://t.co/Kf7uVKekMd #Etymology #words
Another common #question:
What is the difference between “alias” and “pseudonym?”
As nouns alias means “another name; an assumed name,” while pseudonym means “a fictitious name (more literally, a false name), as those used by writers and movie
Here is a very basic #comparison: "Name versus Stage Name"
As #nouns, the difference is that name means “any nounal word or phrase which indicates a particular person, place, class, or thing,” but stage name means “the pseudonym of an
Here's the most useful #Factualist comparison pages #Thread 🧵
What is the difference between “pseudonym” and “stage name?”
Pseudonym means “a fictitious name (more literally, a false name), as those used by writers and movie stars,” while stage name is “the pseudonym of an entertainer.”
https://t.co/hT5XPkTepy #english #wiki #wikidiff
People also found this comparison helpful:
Alias #versus Stage Name: What’s the difference?
Alias means “another name; an assumed name,” while stage name means “the pseudonym of an entertainer.”
https://t.co/Kf7uVKekMd #Etymology #words
Another common #question:
What is the difference between “alias” and “pseudonym?”
As nouns alias means “another name; an assumed name,” while pseudonym means “a fictitious name (more literally, a false name), as those used by writers and movie
Here is a very basic #comparison: "Name versus Stage Name"
As #nouns, the difference is that name means “any nounal word or phrase which indicates a particular person, place, class, or thing,” but stage name means “the pseudonym of an

I held back from commenting overnight to chew it over, but I am still saddened by comments during a presentation I attended yesterday by Prof @trishgreenhalgh & @CIHR_IMHA.
The topic was “LongCovid, Myalgic Encephalomyelitis & More”.
I quote from memory.
1/n
#MECFS #LongCovid
The bulk of Prof @Trishgreenhalgh’s presentation was on the importance of recognising LongCovid patient’s symptoms, and pathways for patients which recognised their condition as real. So far so good.
She was asked about “Post Exertional Malaise”... 2/n
PEM has been reported by many patients, and is the hallmark symptom of ME/CFS, leading many to query whether LongCovid and ME/CFS are similar or have overlapping mechanisms.
@Trishgreenhalgh acknowledged the new @NiceComms advice for LongCovid was planned to complement... 3/n
the ME/CFS guidelines, acknowledging some similarities.
Then it all went wrong.
@TrishGreenhalgh noted the changes to the @NiceComms guidance for ME/CFS, removing support for Graded Exercise Therapy / Cognitive Behavioural Therapy. She noted there is a big debate about this. 4/n
That is correct: The BMJ published Prof Lynne Turner Stokes’ column criticising the change (Prof Turner-Stokes is a key proponent of GET/CBT, and I suspect is known to Prof @TrishGreenhalgh).
https://t.co/0enH8TFPoe
However Prof Greenhalgh then went off-piste.
5/n
The topic was “LongCovid, Myalgic Encephalomyelitis & More”.
I quote from memory.
1/n
#MECFS #LongCovid
Have you registered for IMHA's next webinar on Long-COVID? Guest speaker Professor Trisha Greenhalgh.
— CIHR-IMHA Community (@CIHR_IMHA) January 12, 2021
When? Tomorrow: *Jan 13th.* 12pm ET
A few spots are left, but going fast!
Registration required: https://t.co/T4PbWNA35Y@KarimKhan_IMHA @CIHR_IRSC @trishgreenhalgh pic.twitter.com/xlWKi4QKF1
The bulk of Prof @Trishgreenhalgh’s presentation was on the importance of recognising LongCovid patient’s symptoms, and pathways for patients which recognised their condition as real. So far so good.
She was asked about “Post Exertional Malaise”... 2/n
PEM has been reported by many patients, and is the hallmark symptom of ME/CFS, leading many to query whether LongCovid and ME/CFS are similar or have overlapping mechanisms.
@Trishgreenhalgh acknowledged the new @NiceComms advice for LongCovid was planned to complement... 3/n
the ME/CFS guidelines, acknowledging some similarities.
Then it all went wrong.
@TrishGreenhalgh noted the changes to the @NiceComms guidance for ME/CFS, removing support for Graded Exercise Therapy / Cognitive Behavioural Therapy. She noted there is a big debate about this. 4/n
That is correct: The BMJ published Prof Lynne Turner Stokes’ column criticising the change (Prof Turner-Stokes is a key proponent of GET/CBT, and I suspect is known to Prof @TrishGreenhalgh).
https://t.co/0enH8TFPoe
However Prof Greenhalgh then went off-piste.
5/n



Normally I enjoy the high standards of journalism in @guardian . Not today as disappointed with misleading headline that suggest infections are spreading fastest in children. It'll worry parents/teachers & I doubt most readers will unpick the
The latest REACT1 report shows prevalence of infection in ALL age groups has fallen, including children aged 5-12 from 1.59% in Round 8 to 0.86% in Round 9a. The authors of REACT1 report also (wisely) didn't try to interpret the prevalence figures.
If this were a research trial you wouldn't place much weight on the age differences in % prevalence because of the wide confidence intervals, i.e. differences weren't statistically significant.
3/
I've previously tweeted on the challenges (& dangers) of interpreting surveillance data. One would need lots more contextual info to make sense of it & arrive at sound
Undoubtedly some will extrapolate from the prevalence of infection figures in children to other settings i.e. schools based on the headline. I'd advise caution as there is a real risk of over-interpretation through extrapolation of limited data. Association is not causation.
5/
The latest REACT1 report shows prevalence of infection in ALL age groups has fallen, including children aged 5-12 from 1.59% in Round 8 to 0.86% in Round 9a. The authors of REACT1 report also (wisely) didn't try to interpret the prevalence figures.
If this were a research trial you wouldn't place much weight on the age differences in % prevalence because of the wide confidence intervals, i.e. differences weren't statistically significant.
3/
I've previously tweeted on the challenges (& dangers) of interpreting surveillance data. One would need lots more contextual info to make sense of it & arrive at sound
Misinterpretation of surveillance data is a serious issue. Surveillance data needs to come with a warning label - Open to biases - interpret with caution! Some may not realize that surveillance often does not measure all infection, it's a proxy for actual disease incidence.
— Andrew Lee (@andrewleedr) February 14, 2021
1/
Undoubtedly some will extrapolate from the prevalence of infection figures in children to other settings i.e. schools based on the headline. I'd advise caution as there is a real risk of over-interpretation through extrapolation of limited data. Association is not causation.
5/
You May Also Like






1/12
RT-PCR corona (test) scam
Symptomatic people are tested for one and only one respiratory virus. This means that other acute respiratory infections are reclassified as
2/12
It is tested exquisitely with a hypersensitive non-specific RT-PCR test / Ct >35 (>30 is nonsense, >35 is madness), without considering Ct and clinical context. This means that more acute respiratory infections are reclassified as
3/12
The Drosten RT-PCR test is fabricated in a way that each country and laboratory perform it differently at too high Ct and that the high rate of false positives increases massively due to cross-reaction with other (corona) viruses in the "flu
4/12
Even asymptomatic, previously called healthy, people are tested (en masse) in this way, although there is no epidemiologically relevant asymptomatic transmission. This means that even healthy people are declared as COVID
5/12
Deaths within 28 days after a positive RT-PCR test from whatever cause are designated as deaths WITH COVID. This means that other causes of death are reclassified as
RT-PCR corona (test) scam
Symptomatic people are tested for one and only one respiratory virus. This means that other acute respiratory infections are reclassified as
4/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
...indication, first of all that testing for a (single) respiratory virus is done outside of surveillance systems or need for specific therapy, but even so the lack of consideration of Ct, symptoms and clinical findings when interpreting its result. https://t.co/gHH6kwRdZG
2/12
It is tested exquisitely with a hypersensitive non-specific RT-PCR test / Ct >35 (>30 is nonsense, >35 is madness), without considering Ct and clinical context. This means that more acute respiratory infections are reclassified as
6/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
The neither validated nor standardised hypersensitive RT-PCR test / Ct 35-45 for SARS-CoV-2 is abused to mislabel (also) other diseases, especially influenza, as COVID-19.https://t.co/AkFIfTCTkS
3/12
The Drosten RT-PCR test is fabricated in a way that each country and laboratory perform it differently at too high Ct and that the high rate of false positives increases massively due to cross-reaction with other (corona) viruses in the "flu
External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results.https://t.co/mbNY8bdw1p pic.twitter.com/OQBD4grMth
— Dr. Thomas Binder, MD (@Thomas_Binder) November 29, 2020
4/12
Even asymptomatic, previously called healthy, people are tested (en masse) in this way, although there is no epidemiologically relevant asymptomatic transmission. This means that even healthy people are declared as COVID
Thread web\u2b06\ufe0f\u2b07\ufe0f
— Dr. Thomas Binder, MD (@Thomas_Binder) December 16, 2020
The fabrication of the "asymptomatic (super) spreader" is the coronation of the total nons(ci)ense in the belief system of #CoronasWitnesses.
Asymptomatic transmission 0.7%; 95% CI 0%-4.9% - could well be 0%!https://t.co/VeZTzxXfvT
5/12
Deaths within 28 days after a positive RT-PCR test from whatever cause are designated as deaths WITH COVID. This means that other causes of death are reclassified as
8/8
— Dr. Thomas Binder, MD (@Thomas_Binder) March 24, 2020
By the way, who the f*** created this obviously (almost) worldwide definition of #CoronaDeath?
This is not only medical malpractice, this is utterly insane!https://t.co/FFsTx4L2mw







