
She was asked about “Post Exertional Malaise”... 2/n
I held back from commenting overnight to chew it over, but I am still saddened by comments during a presentation I attended yesterday by Prof @trishgreenhalgh & @CIHR_IMHA.
The topic was “LongCovid, Myalgic Encephalomyelitis & More”.
I quote from memory.
1/n
#MECFS #LongCovid
Have you registered for IMHA's next webinar on Long-COVID? Guest speaker Professor Trisha Greenhalgh.
— CIHR-IMHA Community (@CIHR_IMHA) January 12, 2021
When? Tomorrow: *Jan 13th.* 12pm ET
A few spots are left, but going fast!
Registration required: https://t.co/T4PbWNA35Y@KarimKhan_IMHA @CIHR_IRSC @trishgreenhalgh pic.twitter.com/xlWKi4QKF1
She was asked about “Post Exertional Malaise”... 2/n
@Trishgreenhalgh acknowledged the new @NiceComms advice for LongCovid was planned to complement... 3/n
Then it all went wrong.
@TrishGreenhalgh noted the changes to the @NiceComms guidance for ME/CFS, removing support for Graded Exercise Therapy / Cognitive Behavioural Therapy. She noted there is a big debate about this. 4/n
https://t.co/0enH8TFPoe
However Prof Greenhalgh then went off-piste.
5/n
6/n
Aside from ethical issues of naming patients, this is an n=1 case.
7/n
Furthermore, @TrishGreenhalgh failed to mention Prof Jonathan Edwards’ (not on twitter) Expert Testimony.
8/n
His testimony can be found here:
https://t.co/qLhsBJ4Bcu
9/n
I find this ill-befitting of an academic of her standing.
10/n
It puts her view in the field of politics not medicine.
That opens her to political-style criticism, which would be a shame.
11/n
We must play the ball, not the player.
12/n
Perhaps that is why, between 2015-2016 only £5m / year was spent on researching the condition.
Or aproximatly £0.35p per person, per year. Ouch.
https://t.co/TUPEiSCLZq
13/n
It really hurts.
And how ‘aggressive’ were these patients? Is this tweet aggressive? Will I be blocked and blamed?
14/n
I have a fatiguing gut condition and was mis-diagnosed with ME/CFS 4 years ago. I walked 6Km / day.
A specialist ‘undiagnosed’ me as I did not have PEM.
But in 2005, could I have been eligible for a GET study, and might have felt better after exercise.
15/n
She likes to go for walks, and exercises when she can. Had she taken up the offer to participate in a trial, she may have improved too.
16/n
I also experienced gas-lighting from the 20+ docs who told me it was all in my head. Thankfully I now have much better medical support, but many struggle.
17/n
The condition needs research, and that starts with belief, and develops with high-quality, objective science.
END/
I am actually a big supporter of Prof Greenhalgh’s work. Masks are good. So is good patient care.
I have no malicious intent, but it is right to challenge bad pronouncements on this issue.

If you think I have got it wrong, please let me know.
Please challenge misinformation about on ME/CFS, but accept that even great people make mistakes. Forgive.
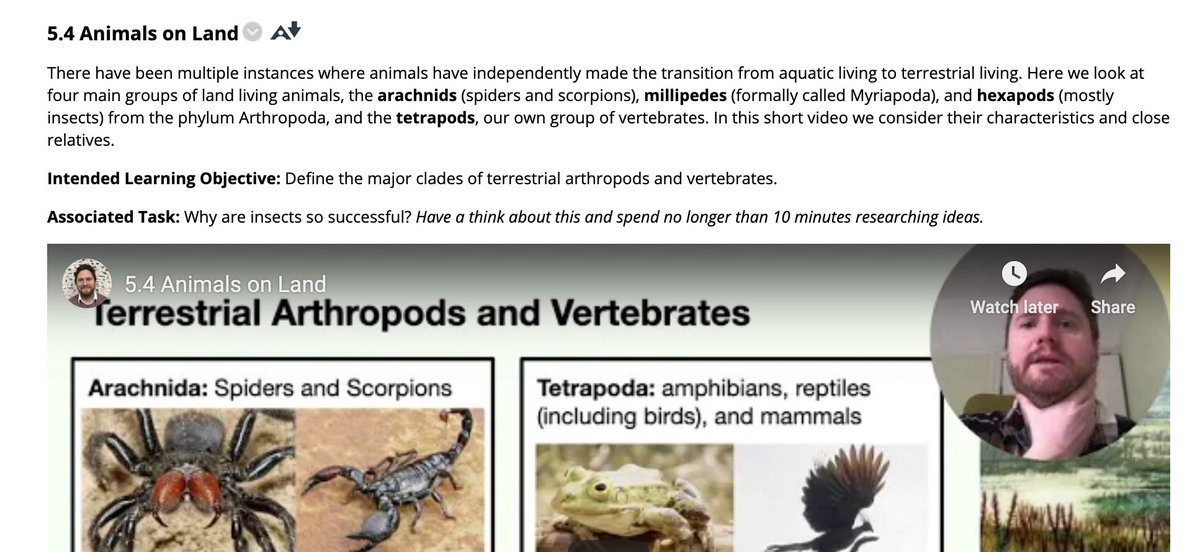
More from Education


Time for some thoughts on schools given the revised SickKids document and the fact that ON decided to leave most schools closed. ON is not the only jurisdiction to do so, but important to note that many jurisdictions would not have done so -even with higher incidence rates.
As outlined in the tweet by @NishaOttawa yesterday, the situation is complex, and not a simple right or wrong https://t.co/DO0v3j9wzr. And no one needs to list all the potential risks and downsides of prolonged school closures.
On the other hand: while school closures do not directly protect our most vulnerable in long-term care at all, one cannot deny that any factor potentially increasing community transmission may have an indirect effect on the risk to these institutions, and on healthcare.
The question is: to what extend do schools contribute to transmission, and how to balance this against the risk of prolonged school closures. The leaked data from yesterday shows a mixed picture -schools are neither unicorns (ie COVID free) nor infernos.
Assuming this data is largely correct -while waiting for an official publication of the data, it shows first and foremost the known high case numbers at Thorncliff, while other schools had been doing very well -are safe- reiterating the impact of socioeconomics on the COVID risk.
A group of Ontario experts led by SickKids has updated its guidance for school operation during the COVID-19 pandemic. The living document, COVID-19: Updated Guidance for School Operation During the Pandemic, can be read here: https://t.co/rotLqDqkQh pic.twitter.com/q7kVezAPoG
— SickKids_TheHospital (@SickKidsNews) January 21, 2021
As outlined in the tweet by @NishaOttawa yesterday, the situation is complex, and not a simple right or wrong https://t.co/DO0v3j9wzr. And no one needs to list all the potential risks and downsides of prolonged school closures.
1/It's the eve of provincial announcements on schools reopening for in-person instruction.
— Nisha Thampi (@NishaOttawa) January 20, 2021
Households are under stress and experts are divided on whether schools are unicorns or infernos.
Everyone wants to do right by kids, who have borne so much throughout this pandemic.
On the other hand: while school closures do not directly protect our most vulnerable in long-term care at all, one cannot deny that any factor potentially increasing community transmission may have an indirect effect on the risk to these institutions, and on healthcare.
The question is: to what extend do schools contribute to transmission, and how to balance this against the risk of prolonged school closures. The leaked data from yesterday shows a mixed picture -schools are neither unicorns (ie COVID free) nor infernos.
Assuming this data is largely correct -while waiting for an official publication of the data, it shows first and foremost the known high case numbers at Thorncliff, while other schools had been doing very well -are safe- reiterating the impact of socioeconomics on the COVID risk.

Our top 15 tweets
A #prodmgmt thread 👇
https://t.co/Yv854Sd3P3
https://t.co/sXaMH1bZ9m
https://t.co/5X7bOTsS7m
https://t.co/w1y6LTtPS2
A #prodmgmt thread 👇
https://t.co/Yv854Sd3P3
Sum up Product Management in 4 words or less. \U0001f609
— Product School (@productschool) April 10, 2020
https://t.co/sXaMH1bZ9m
\u201cWithout data, you\u2019re just another person with an opinion.\u201d
— Product School (@productschool) July 22, 2020
-W. Edwards Deming
https://t.co/5X7bOTsS7m
MVP (Minimum Viable Product) or MLP (Minimum Lovable Product)? \u2764\ufe0f
— Product School (@productschool) July 6, 2020
https://t.co/w1y6LTtPS2
UI/UX are not just add-ons for a product. They\u2019re critical elements that need care, research, and a Product Manager\u2019s full attention.
— Product School (@productschool) July 12, 2020


Normally I enjoy the high standards of journalism in @guardian . Not today as disappointed with misleading headline that suggest infections are spreading fastest in children. It'll worry parents/teachers & I doubt most readers will unpick the
The latest REACT1 report shows prevalence of infection in ALL age groups has fallen, including children aged 5-12 from 1.59% in Round 8 to 0.86% in Round 9a. The authors of REACT1 report also (wisely) didn't try to interpret the prevalence figures.
If this were a research trial you wouldn't place much weight on the age differences in % prevalence because of the wide confidence intervals, i.e. differences weren't statistically significant.
3/
I've previously tweeted on the challenges (& dangers) of interpreting surveillance data. One would need lots more contextual info to make sense of it & arrive at sound
Undoubtedly some will extrapolate from the prevalence of infection figures in children to other settings i.e. schools based on the headline. I'd advise caution as there is a real risk of over-interpretation through extrapolation of limited data. Association is not causation.
5/
The latest REACT1 report shows prevalence of infection in ALL age groups has fallen, including children aged 5-12 from 1.59% in Round 8 to 0.86% in Round 9a. The authors of REACT1 report also (wisely) didn't try to interpret the prevalence figures.
If this were a research trial you wouldn't place much weight on the age differences in % prevalence because of the wide confidence intervals, i.e. differences weren't statistically significant.
3/
I've previously tweeted on the challenges (& dangers) of interpreting surveillance data. One would need lots more contextual info to make sense of it & arrive at sound
Misinterpretation of surveillance data is a serious issue. Surveillance data needs to come with a warning label - Open to biases - interpret with caution! Some may not realize that surveillance often does not measure all infection, it's a proxy for actual disease incidence.
— Andrew Lee (@andrewleedr) February 14, 2021
1/
Undoubtedly some will extrapolate from the prevalence of infection figures in children to other settings i.e. schools based on the headline. I'd advise caution as there is a real risk of over-interpretation through extrapolation of limited data. Association is not causation.
5/
You May Also Like

🌿𝑻𝒉𝒆 𝒔𝒕𝒐𝒓𝒚 𝒐𝒇 𝒂 𝑺𝒕𝒂𝒓 : 𝑫𝒉𝒓𝒖𝒗𝒂 & 𝑽𝒊𝒔𝒉𝒏𝒖
Once upon a time there was a Raja named Uttānapāda born of Svayambhuva Manu,1st man on earth.He had 2 beautiful wives - Suniti & Suruchi & two sons were born of them Dhruva & Uttama respectively.
#talesofkrishna https://t.co/E85MTPkF9W
Now Suniti was the daughter of a tribal chief while Suruchi was the daughter of a rich king. Hence Suruchi was always favored the most by Raja while Suniti was ignored. But while Suniti was gentle & kind hearted by nature Suruchi was venomous inside.
#KrishnaLeela
The story is of a time when ideally the eldest son of the king becomes the heir to the throne. Hence the sinhasan of the Raja belonged to Dhruva.This is why Suruchi who was the 2nd wife nourished poison in her heart for Dhruva as she knew her son will never get the throne.
One day when Dhruva was just 5 years old he went on to sit on his father's lap. Suruchi, the jealous queen, got enraged and shoved him away from Raja as she never wanted Raja to shower Dhruva with his fatherly affection.
Dhruva protested questioning his step mother "why can't i sit on my own father's lap?" A furious Suruchi berated him saying "only God can allow him that privilege. Go ask him"

Once upon a time there was a Raja named Uttānapāda born of Svayambhuva Manu,1st man on earth.He had 2 beautiful wives - Suniti & Suruchi & two sons were born of them Dhruva & Uttama respectively.
#talesofkrishna https://t.co/E85MTPkF9W
Prabhu says i reside in the heart of my bhakt.
— Right Singh (@rightwingchora) December 21, 2020
Guess the event. pic.twitter.com/yFUmbfe5KL
Now Suniti was the daughter of a tribal chief while Suruchi was the daughter of a rich king. Hence Suruchi was always favored the most by Raja while Suniti was ignored. But while Suniti was gentle & kind hearted by nature Suruchi was venomous inside.
#KrishnaLeela
The story is of a time when ideally the eldest son of the king becomes the heir to the throne. Hence the sinhasan of the Raja belonged to Dhruva.This is why Suruchi who was the 2nd wife nourished poison in her heart for Dhruva as she knew her son will never get the throne.
One day when Dhruva was just 5 years old he went on to sit on his father's lap. Suruchi, the jealous queen, got enraged and shoved him away from Raja as she never wanted Raja to shower Dhruva with his fatherly affection.
Dhruva protested questioning his step mother "why can't i sit on my own father's lap?" A furious Suruchi berated him saying "only God can allow him that privilege. Go ask him"



First update to https://t.co/lDdqjtKTZL since the challenge ended – Medium links!! Go add your Medium profile now 👀📝 (thanks @diannamallen for the suggestion 😁)

Just added Telegram links to https://t.co/lDdqjtKTZL too! Now you can provide a nice easy way for people to message you :)

Less than 1 hour since I started adding stuff to https://t.co/lDdqjtKTZL again, and profile pages are now responsive!!! 🥳 Check it out -> https://t.co/fVkEL4fu0L
Accounts page is now also responsive!! 📱✨
💪 I managed to make the whole site responsive in about an hour. On my roadmap I had it down as 4-5 hours!!! 🤘🤠🤘
Just added Telegram links to https://t.co/lDdqjtKTZL too! Now you can provide a nice easy way for people to message you :)
Less than 1 hour since I started adding stuff to https://t.co/lDdqjtKTZL again, and profile pages are now responsive!!! 🥳 Check it out -> https://t.co/fVkEL4fu0L
Accounts page is now also responsive!! 📱✨
💪 I managed to make the whole site responsive in about an hour. On my roadmap I had it down as 4-5 hours!!! 🤘🤠🤘
