
How did it come to this? A deeply misguided effort (@joyhataley) to silence @randyhillier, a MPP in the provincial legislature. This reflects poorly on the medical community. How could one do it differently in a thoughtful, educated manner. Lets consider. 1/
It\u2019s time to sign!
— Dr. Joy Hataley (@JoyHataley) January 3, 2021
Your nurse and your doctor are!@RNAO@OntariosDoctors @CMAJ @MedicalPost @CKWS_TV @ctvottawa @CTVToronto @CTVToronto @MOHKFLA https://t.co/IPHbuBkuJW
https://t.co/IJiFPL3FWX
Twelve Forgotten Principles of Public Health
— Martin Kulldorff (@MartinKulldorff) December 19, 2020
#1 Public health is about all health outcomes, not just a single disease like #COVID19. It is important to also consider harms from public health measures. #totalharmshttps://t.co/JSlZ5K23mp @collateralglbl
https://t.co/OHQc6gdldm

More from Health



This is a limited point about availability of efficacy data for vaccines under development in the context of the approval for CovidShield and Covaxin in India.
There have been many so-called experts on the idiotbox opining about apparent availability of P III data which 1/n
2/n apparently the SEC had access to based on which it "supposedly" approved Covaxin. Another argument that is prevalent is other regulators (US FDA and MHRA) also approved vaccines based on P II data alone. Let me give you a few facts so that you can make your own decision.
3/n The protocols for both mRNA vaccines are publicly available. You can check. Both protocols *define* when the interim analysis will be done. This is not subjective. They clearly define how many infections need to be documented before the Data Safety Monitoring Board meets.
4/n Find the protocols for the bridging study for CovidShield and Covaxin and look for a similar milestone.
Here is one set of efficacy data post the interim analysis of a mRNA vaccine.
Source: https://t.co/BAPnP3PxEb
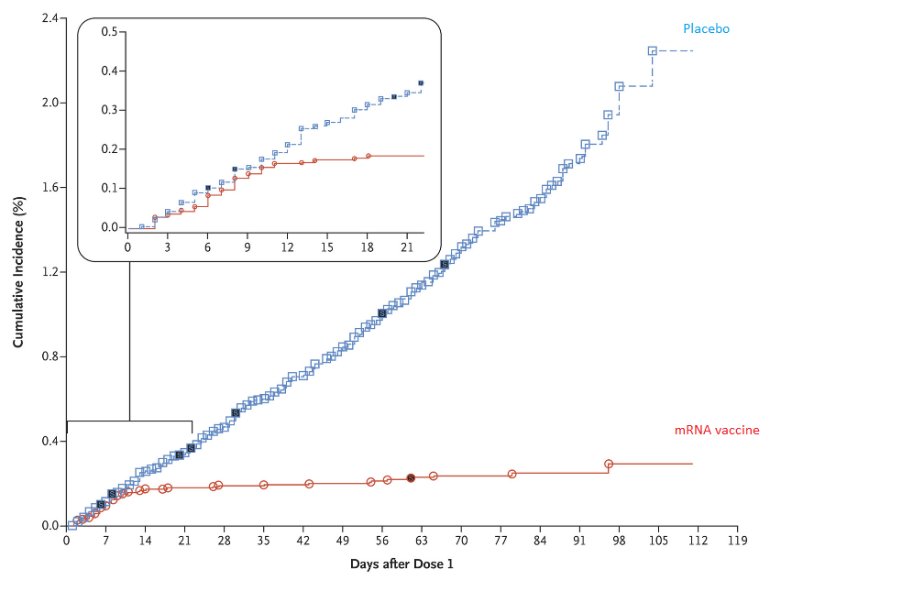
5/n This data was analyzed post the interim analysis where the blind was broken by the DSMB. Now ask yourself this question:
How does the SEC, or the sponsor of these studies, or the experts who are offering their opinion liberally on the idiotbox know what the efficacy is
There have been many so-called experts on the idiotbox opining about apparent availability of P III data which 1/n
2/n apparently the SEC had access to based on which it "supposedly" approved Covaxin. Another argument that is prevalent is other regulators (US FDA and MHRA) also approved vaccines based on P II data alone. Let me give you a few facts so that you can make your own decision.
3/n The protocols for both mRNA vaccines are publicly available. You can check. Both protocols *define* when the interim analysis will be done. This is not subjective. They clearly define how many infections need to be documented before the Data Safety Monitoring Board meets.
4/n Find the protocols for the bridging study for CovidShield and Covaxin and look for a similar milestone.
Here is one set of efficacy data post the interim analysis of a mRNA vaccine.
Source: https://t.co/BAPnP3PxEb
5/n This data was analyzed post the interim analysis where the blind was broken by the DSMB. Now ask yourself this question:
How does the SEC, or the sponsor of these studies, or the experts who are offering their opinion liberally on the idiotbox know what the efficacy is

I applaud the #EUCancerPlan *BUT* caution: putting #meat 🥩 (a nourishing, evolutionary food) in the same box as 🚬 to solve a contemporary health challenge, would be basing policy on assumptions rather than robust data.
#FollowTheScience yes, but not just part of it!
THREAD👇
1/ Granted, some studies have pointed to ASSOCIATIONS of HIGH intake of red & processed meats with (slightly!) increased colorectal cancer incidence. Also, @WHO/IARC is often mentioned in support (usually hyperbolically so).
But, let’s have a closer look at all this! 🔍

2/ First, meat being “associated” with cancer is very different from stating that meat CAUSES cancer.
Unwarranted use of causal language is widespread in nutritional sciences, posing a systemic problem & undermining credibility.
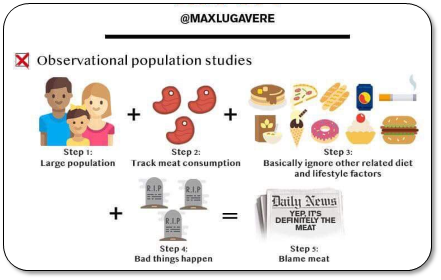
3/ That’s because observational data are CONFOUNDED (even after statistical adjustment).
Healthy user bias is a major problem. Healthy middle classes are TOLD to eat less red meat (due to historical rather than rational reasons, cf link). So, they
4/ What’s captured here is sociology, not physiology.
Health-focused Westerners eat less red meat, whereas those who don’t adhere to dietary advice tend to have unhealthier lifestyles.
That tells us very little about meat AS SUCH being responsible for disease.
#FollowTheScience yes, but not just part of it!
THREAD👇
\U0001f534LIVE \U0001f4c5Today \u23f012:00 CET
— EU_HEALTH - #EUCancerPlan (@EU_Health) February 3, 2021
We are presenting today the #EUCancerPlan as part of a strong \U0001f1ea\U0001f1fa#HealthUnion
Follow the presentation live here: https://t.co/Cr8ATvzNkg#WorldCancerDay pic.twitter.com/zdByuklWV6
1/ Granted, some studies have pointed to ASSOCIATIONS of HIGH intake of red & processed meats with (slightly!) increased colorectal cancer incidence. Also, @WHO/IARC is often mentioned in support (usually hyperbolically so).
But, let’s have a closer look at all this! 🔍
2/ First, meat being “associated” with cancer is very different from stating that meat CAUSES cancer.
Unwarranted use of causal language is widespread in nutritional sciences, posing a systemic problem & undermining credibility.
3/ That’s because observational data are CONFOUNDED (even after statistical adjustment).
Healthy user bias is a major problem. Healthy middle classes are TOLD to eat less red meat (due to historical rather than rational reasons, cf link). So, they
4/ What’s captured here is sociology, not physiology.
Health-focused Westerners eat less red meat, whereas those who don’t adhere to dietary advice tend to have unhealthier lifestyles.
That tells us very little about meat AS SUCH being responsible for disease.















