
This is a limited point about availability of efficacy data for vaccines under development in the context of the approval for CovidShield and Covaxin in India.
There have been many so-called experts on the idiotbox opining about apparent availability of P III data which 1/n
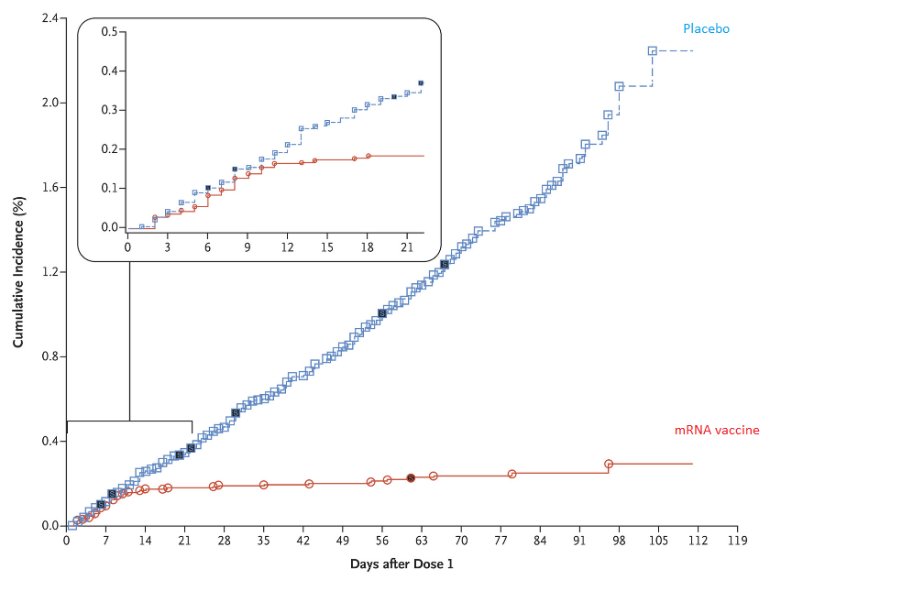
Here is one set of efficacy data post the interim analysis of a mRNA vaccine.
Source: https://t.co/BAPnP3PxEb
How does the SEC, or the sponsor of these studies, or the experts who are offering their opinion liberally on the idiotbox know what the efficacy is
A. Do they know if the blind was broken for the bridging study and the Phase III study?
B. If so, can they produce data like the one above showing how many subjects who were infected were
And if they cannot answer this question, then ask the following question:
C. In the absence of efficacy data, how does one claim that the vaccine candidate is effective?
D. Do they agree that therapeutic candidates ought to be approved
More from Health

🚨New lockdown regulations just published, in force tomorrow
The Health Protection (Coronavirus, Restrictions) (No. 3) and (All Tiers) (England) (Amendment) Regulations 2021
https://t.co/L5jwlTDaIE
(Thread)
These are not a new set of regulations: they are amendments an old set of regulations
Which we thought were gone! But they are back
Welcome back No.3 regulations
A quick thing before we continue!
I have been analysing these laws for free for 9 months now - if you want to say thanks and have a few £ to spare please give to my @LawCentres fundraiser
They give free legal advice to people who need it
They also amend the All Tiers regulations
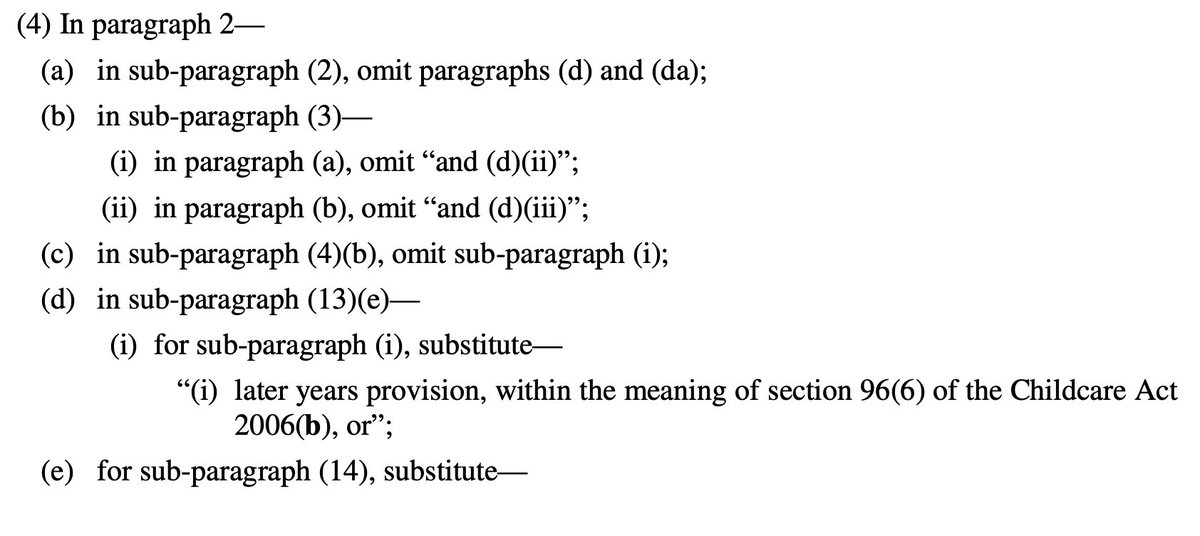
Oh god it's all amendments by paragraph references
Basically all of England now in Tier 4 and Tier 4 is amended but not by a huge amount
This really is a terrible way to make laws on the fly - who can possibly understand it?!
So, to explain, you need 2 documents open if you want to understand what is going on:
All Tiers regulations (Tiers 1-4, 2 December as amended) https://t.co/IraPQ112ak
And amendments https://t.co/L5jwlTDaIE
No sensible way of doing except by track changes, on it now, back soon
The Health Protection (Coronavirus, Restrictions) (No. 3) and (All Tiers) (England) (Amendment) Regulations 2021
https://t.co/L5jwlTDaIE
(Thread)
These are not a new set of regulations: they are amendments an old set of regulations
Which we thought were gone! But they are back
Welcome back No.3 regulations
A quick thing before we continue!
I have been analysing these laws for free for 9 months now - if you want to say thanks and have a few £ to spare please give to my @LawCentres fundraiser
They give free legal advice to people who need it
They also amend the All Tiers regulations
Oh god it's all amendments by paragraph references
Basically all of England now in Tier 4 and Tier 4 is amended but not by a huge amount
This really is a terrible way to make laws on the fly - who can possibly understand it?!
So, to explain, you need 2 documents open if you want to understand what is going on:
All Tiers regulations (Tiers 1-4, 2 December as amended) https://t.co/IraPQ112ak
And amendments https://t.co/L5jwlTDaIE
No sensible way of doing except by track changes, on it now, back soon







Thread on how atheism leads to mental retardation (backed with medical citations🧵💉)
To start with, atheism is an unnatural self-contradicting doctrine.
Medical terminology proves that human beings are naturally pre-disposed to believe in God. Oxford scientists assert that people are "born believers".
https://t.co/kE0Fi588yn
https://t.co/OqyXcGIMJn

It should be known that atheism could never produce an intelligently-functioning society and neither ever will.
Contrastingly, Islam produced several intellectuals & polymaths, was on the forefront of scientific development, boasting 100% literacy
It is also scientifically proven that atheism led to lesser scientific curiosity and scientific frauds, which is also why atheists incline to pseudo-science.
Whereas, religion in general and Islam in particular boosted education.
https://t.co/19Onc84u3g

Atheists are also likely to affected by pervasive mental and developmental disorders like high-functioning autism.
Cognitive Scientists and renowned Neurologists found that more atheism is leads to greater autism.
https://t.co/zRjEyFoX3P

To start with, atheism is an unnatural self-contradicting doctrine.
Medical terminology proves that human beings are naturally pre-disposed to believe in God. Oxford scientists assert that people are "born believers".
https://t.co/kE0Fi588yn
https://t.co/OqyXcGIMJn
It should be known that atheism could never produce an intelligently-functioning society and neither ever will.
Contrastingly, Islam produced several intellectuals & polymaths, was on the forefront of scientific development, boasting 100% literacy
If the Muslim world had not existed, there literally would be no technology/achievements today.
— Starks\u262a\ufe0f\U0001f1f9\U0001f1e9 (@MegaIntelIect) January 8, 2021
Science only developed because of Islam, Europe should be grateful to Islam for civilizing their barbaric cult.
Source: The Caliph's Splendor, Pg 204-05 https://t.co/HVypO52Tpc pic.twitter.com/00jYSbaDSs
It is also scientifically proven that atheism led to lesser scientific curiosity and scientific frauds, which is also why atheists incline to pseudo-science.
Whereas, religion in general and Islam in particular boosted education.
https://t.co/19Onc84u3g
Atheists are also likely to affected by pervasive mental and developmental disorders like high-functioning autism.
Cognitive Scientists and renowned Neurologists found that more atheism is leads to greater autism.
https://t.co/zRjEyFoX3P




















