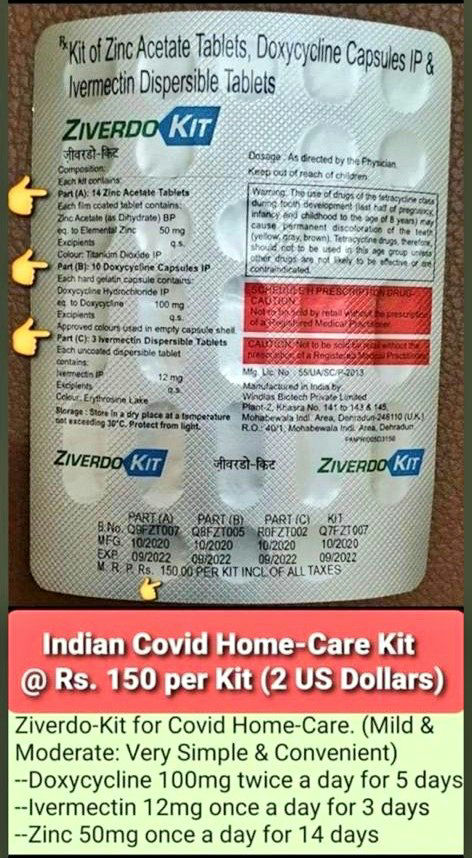
Can any MP ask the government why early treatment kits to stop viral replication & infection are not made available cheaply & prescription free in pharmacies as they are in India? Is it lives we want to save or is it Big Pharma profits? Because the two are mutually exclusive.
More from Robin Monotti
The problem with meta-analysis like this is that it obfuscates the most important issue of treatment, which is timing.
This meta-analysis of controlled trials only looks at hospitalized patients. How long were the patients ill for before being hospitalized? One week? Two? Three? Too late for zinc ionophores (HCQ) (+ZINC? No zinc no point..) to work. Severe illness becomes bacterial in nature.
Was azythromycin administered when the bacterial infections were also too advanced? I have seen Azythromycin work with my very own eyes but that's not to say that if administered too late it may not save the patient. How many patients were given AZT & ventilated? It's all timing.
All the meta-analysis is telling us is if you leave it too late you may have missed the early window for antiviral zinc treatment (Zn+HCQ) & that if you are given AZT when you are ventilated or very severe it may too late for it to save you & corticosteroids may be last resort.
And of course antibiotics need also probiotics, or they may harm the bacterial flora which is part of the immune response. Difficult to tell from a meta-analysis how this problem was managed.
#BMJResearch update: Corticosteroids probably reduce mortality and mechanical ventilation in patients with covid-19 compared with standard care, whereas azithromycin, hydroxychloroquine, interferon-beta, and tocilizumab may not reduce either https://t.co/oQ3lTWUqaz
— The BMJ (@bmj_latest) December 18, 2020
This meta-analysis of controlled trials only looks at hospitalized patients. How long were the patients ill for before being hospitalized? One week? Two? Three? Too late for zinc ionophores (HCQ) (+ZINC? No zinc no point..) to work. Severe illness becomes bacterial in nature.
Was azythromycin administered when the bacterial infections were also too advanced? I have seen Azythromycin work with my very own eyes but that's not to say that if administered too late it may not save the patient. How many patients were given AZT & ventilated? It's all timing.
All the meta-analysis is telling us is if you leave it too late you may have missed the early window for antiviral zinc treatment (Zn+HCQ) & that if you are given AZT when you are ventilated or very severe it may too late for it to save you & corticosteroids may be last resort.
And of course antibiotics need also probiotics, or they may harm the bacterial flora which is part of the immune response. Difficult to tell from a meta-analysis how this problem was managed.
The evidence based science shows that medical face masks for the healthy do not alter rates of community transmission of SARSCoV2 while they contribute to the plastic pollution of planet. Cloth & masks of other materials increase rates of infection through nebulization spread.
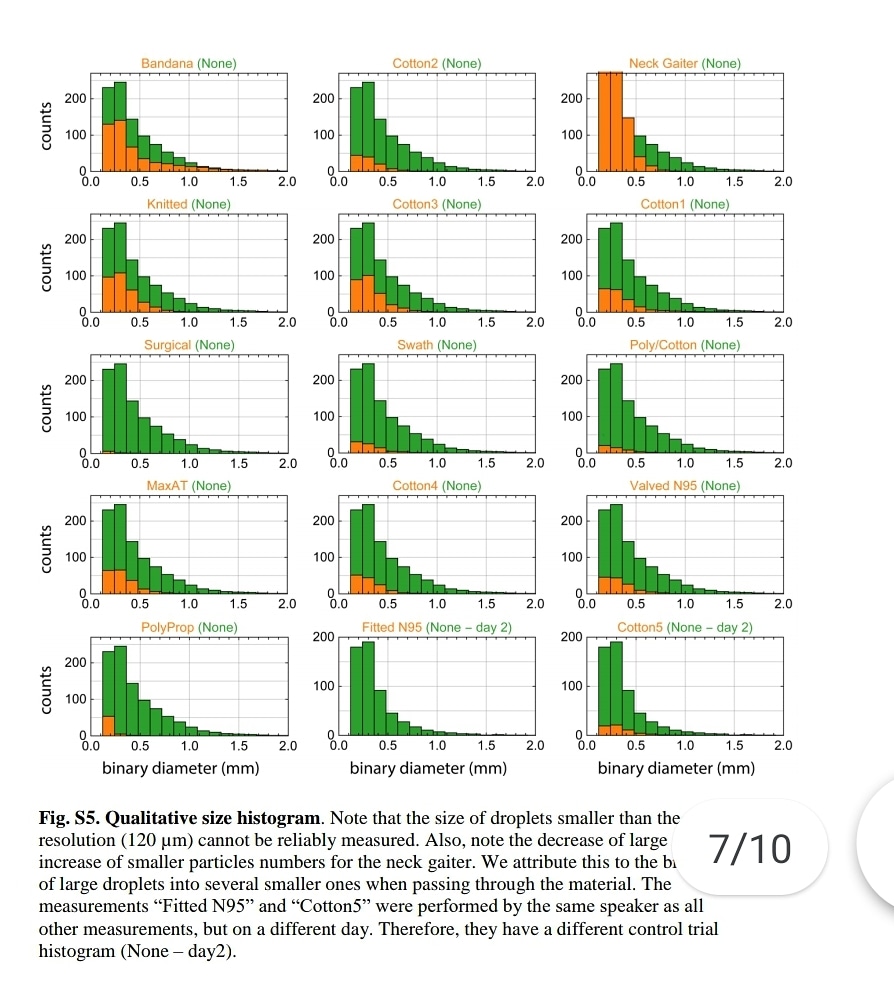
"Speaking through some masks dispersed largest droplets into a multitude of smaller droplets..smaller particles are airborne longer than large droplets (larger droplets sink faster), a mask might be counterproductive."
https://t.co/jBQlWRxcEL
Influenza like illness rates 3 times higher with cloth masks when compared to control group:
https://t.co/djT0mfutv9
Prof. Carl Heneghan, Oxford University: "The high quality trial evidence for cloth masks suggest they increase your rate of reinfection."

Please note, droplets smaller than 120 microns can't be measured. SARSCoV2 is 0.14 microns. This means that the nebulization effect of medical masks could not be measured, not that it does not happen. ⬇️
The really small aerosols <1 μm [the ones that pass through ALL surgical masks] can penetrate all the way to the alveoli - the basic units for gas exchange
"Speaking through some masks dispersed largest droplets into a multitude of smaller droplets..smaller particles are airborne longer than large droplets (larger droplets sink faster), a mask might be counterproductive."
https://t.co/jBQlWRxcEL
Influenza like illness rates 3 times higher with cloth masks when compared to control group:
https://t.co/djT0mfutv9
Prof. Carl Heneghan, Oxford University: "The high quality trial evidence for cloth masks suggest they increase your rate of reinfection."
Please note, droplets smaller than 120 microns can't be measured. SARSCoV2 is 0.14 microns. This means that the nebulization effect of medical masks could not be measured, not that it does not happen. ⬇️
"Speaking through some masks dispersed largest droplets into a multitude of smaller droplets..smaller particles are airborne longer than large droplets (larger droplets sink faster), a mask might be counterproductive."https://t.co/jBQlWRxcEL pic.twitter.com/XeKYFmjsGs
— Robin Monotti (@robinmonotti) January 15, 2021
The really small aerosols <1 μm [the ones that pass through ALL surgical masks] can penetrate all the way to the alveoli - the basic units for gas exchange
4/In humans, larger aerosols deposit in upper throat, nose, & tracheobronchial region of the lung. Medium-sized aerosols mostly deposit in small airways further down. The really small aerosols <1 \u03bcm can penetrate all the way to the alveoli - the basic units for gas exchange. 4/7 pic.twitter.com/9ZJb4JrZqI
— Dr. Ali Nouri (@AliNouriPhD) December 29, 2020
More from Health





Now you know I love to sh-t in Harvard. But I also like accuracy. So I decided to go look at Harvard’s catalog to see its lack of military history that this article describes (they only teach history of pets it claims) and what I found shocked me! Shocked me! A thread: 1/
First off, Harvard students literally have multiple sections of military history that they can take listed. (It appears these ones are taught at MIT, so they might have to walk down the street for these) but... 2/

Say they want to stay on campus...they can only take numerous classes on war and diplomacy...3/
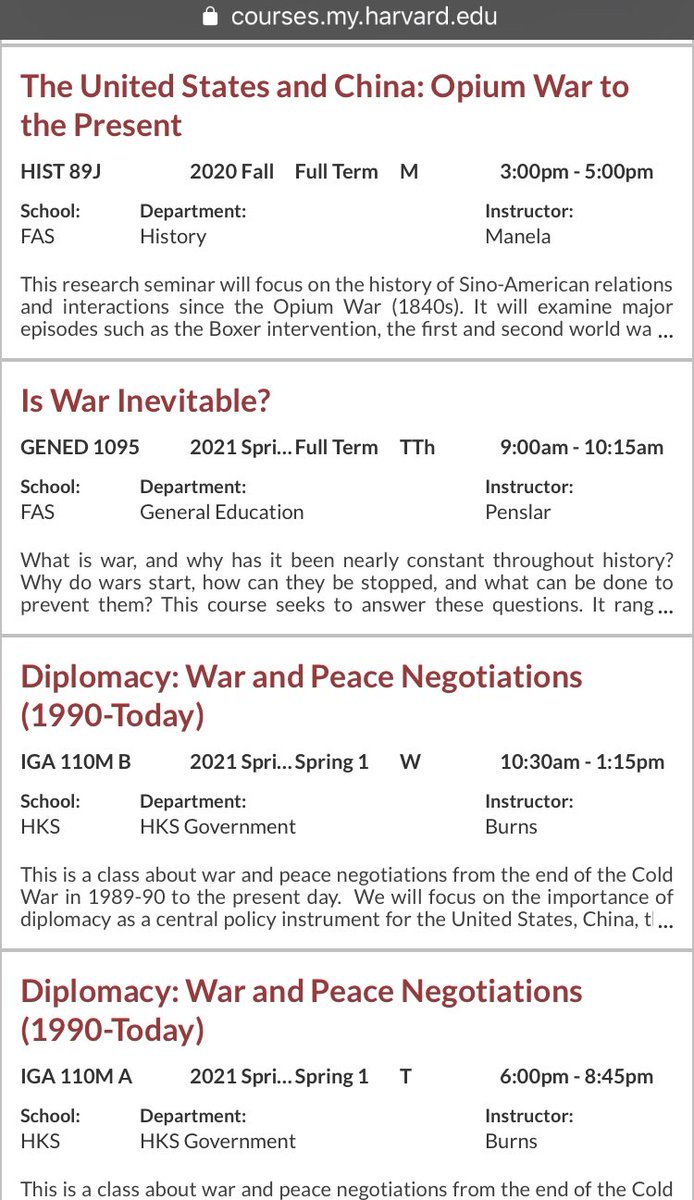
They have an entire class on Yalta. That’s right. An entire class on Yalta. 4/

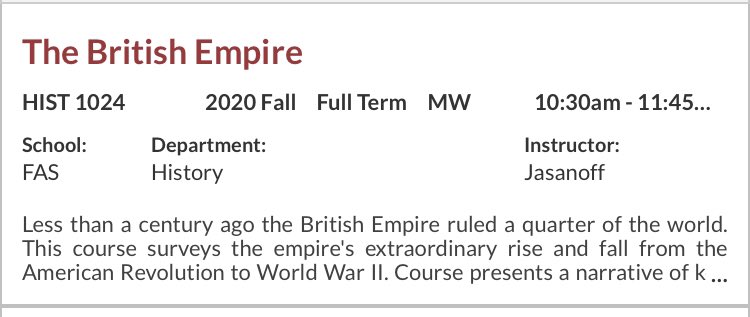
But wait! There is more! They can take the British Empire, The Fall of the Roman Empire for those wanting traditional topics... 5/
\u201cMilitary history\u201d is only in decline if you\u2014like the author & experts in this obnoxious piece\u2014see the subject as a narrowly defined, white dude-oriented, guns & bayonets approach. The field is 1000% better off w/today\u2019s diversity of topics & historians. https://t.co/dUf3OWyVpQ
— Jonathan S. Jones (@_jonathansjones) February 1, 2021
First off, Harvard students literally have multiple sections of military history that they can take listed. (It appears these ones are taught at MIT, so they might have to walk down the street for these) but... 2/
Say they want to stay on campus...they can only take numerous classes on war and diplomacy...3/
They have an entire class on Yalta. That’s right. An entire class on Yalta. 4/
But wait! There is more! They can take the British Empire, The Fall of the Roman Empire for those wanting traditional topics... 5/

I applaud the #EUCancerPlan *BUT* caution: putting #meat 🥩 (a nourishing, evolutionary food) in the same box as 🚬 to solve a contemporary health challenge, would be basing policy on assumptions rather than robust data.
#FollowTheScience yes, but not just part of it!
THREAD👇
1/ Granted, some studies have pointed to ASSOCIATIONS of HIGH intake of red & processed meats with (slightly!) increased colorectal cancer incidence. Also, @WHO/IARC is often mentioned in support (usually hyperbolically so).
But, let’s have a closer look at all this! 🔍

2/ First, meat being “associated” with cancer is very different from stating that meat CAUSES cancer.
Unwarranted use of causal language is widespread in nutritional sciences, posing a systemic problem & undermining credibility.
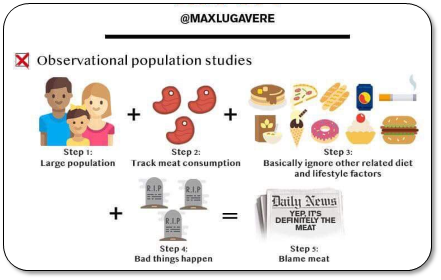
3/ That’s because observational data are CONFOUNDED (even after statistical adjustment).
Healthy user bias is a major problem. Healthy middle classes are TOLD to eat less red meat (due to historical rather than rational reasons, cf link). So, they
4/ What’s captured here is sociology, not physiology.
Health-focused Westerners eat less red meat, whereas those who don’t adhere to dietary advice tend to have unhealthier lifestyles.
That tells us very little about meat AS SUCH being responsible for disease.
#FollowTheScience yes, but not just part of it!
THREAD👇
\U0001f534LIVE \U0001f4c5Today \u23f012:00 CET
— EU_HEALTH - #EUCancerPlan (@EU_Health) February 3, 2021
We are presenting today the #EUCancerPlan as part of a strong \U0001f1ea\U0001f1fa#HealthUnion
Follow the presentation live here: https://t.co/Cr8ATvzNkg#WorldCancerDay pic.twitter.com/zdByuklWV6
1/ Granted, some studies have pointed to ASSOCIATIONS of HIGH intake of red & processed meats with (slightly!) increased colorectal cancer incidence. Also, @WHO/IARC is often mentioned in support (usually hyperbolically so).
But, let’s have a closer look at all this! 🔍
2/ First, meat being “associated” with cancer is very different from stating that meat CAUSES cancer.
Unwarranted use of causal language is widespread in nutritional sciences, posing a systemic problem & undermining credibility.
3/ That’s because observational data are CONFOUNDED (even after statistical adjustment).
Healthy user bias is a major problem. Healthy middle classes are TOLD to eat less red meat (due to historical rather than rational reasons, cf link). So, they
4/ What’s captured here is sociology, not physiology.
Health-focused Westerners eat less red meat, whereas those who don’t adhere to dietary advice tend to have unhealthier lifestyles.
That tells us very little about meat AS SUCH being responsible for disease.