CodyyyGardner Categories Health






So, in terms of people in Melbourne freaking out about Sydney's seemingly lacking response to the current outbreak, coupled with the new cases in Victoria - this is going to trigger a trauma response.
The lockdown was traumatising.
How much, depends on the individual.
When you have a trauma response, it is physically terrifying. Your adrenaline might surge. You could feel afraid. You could feel angry. You might react by lashing out. You might shut down. You might have anxiety that it is all "going to happen again".
Or that you don't think you could survive another lockdown, because you barely survived the last one.
These are all natural and normal responses, and I know they are hard, and I am so sorry if you're feeling this fear.
I don't know what is going to happen.
I do hope that you can do your best to be safe. Try to take each moment as it comes, do the best you can do to get by.
Please find helplines below.
Beyond Blue Covid Mental Health call 1800 512 348 (also online
Australians, this time of year is extremely difficult for many people. A thread (in progress) for contacts;
— MJ Leaver (@MJ_Leaver) December 18, 2017
000 if life is in danger.
1300 659 467 : National Suicide Call Back Service (15+)
1800 55 1800 : Kid's Helpline (5-25yrs)
1800 184 527 : QLife (LGBTQI folks)



A well-balanced piece. Bed occupancy rate in NHS is actually lower than usual - even with fewer beds. (Though spare capacity has been created through cancellation of non-urgent operations etc, and higher levels of staff sickness are causing pressures.) https://t.co/CH8hGcFOs9
— Paul Embery (@PaulEmbery) January 8, 2021
Under normal circumstances, most NHS acute hospitals will have several types of inpatient areas
1. Assessment unit
2. Specialty wards
3. Intensive care
As well as outpatients, emergency department, day case surgery etc.
Patients admitted from A&E would go to 1, then move to 2. Some might go directly to 2, sickest ones to 3.
In many hospitals, the assessment unit is vital to flow of patients out of Emergency Department.
With COVID, several blocks have been introduced. Firstly patients have to be treated as "hot" in 2m apart bed spaces until their test results are back. This reduces an average six bedded bay to four.
There are rapid tests that turn around in around an hour or two, but their availability is limited. PCR still takes up to 24 hours to get back (often quicker), and lateral flow in the population admitted to hospital isn't sensitive enough to pick up silent cases.










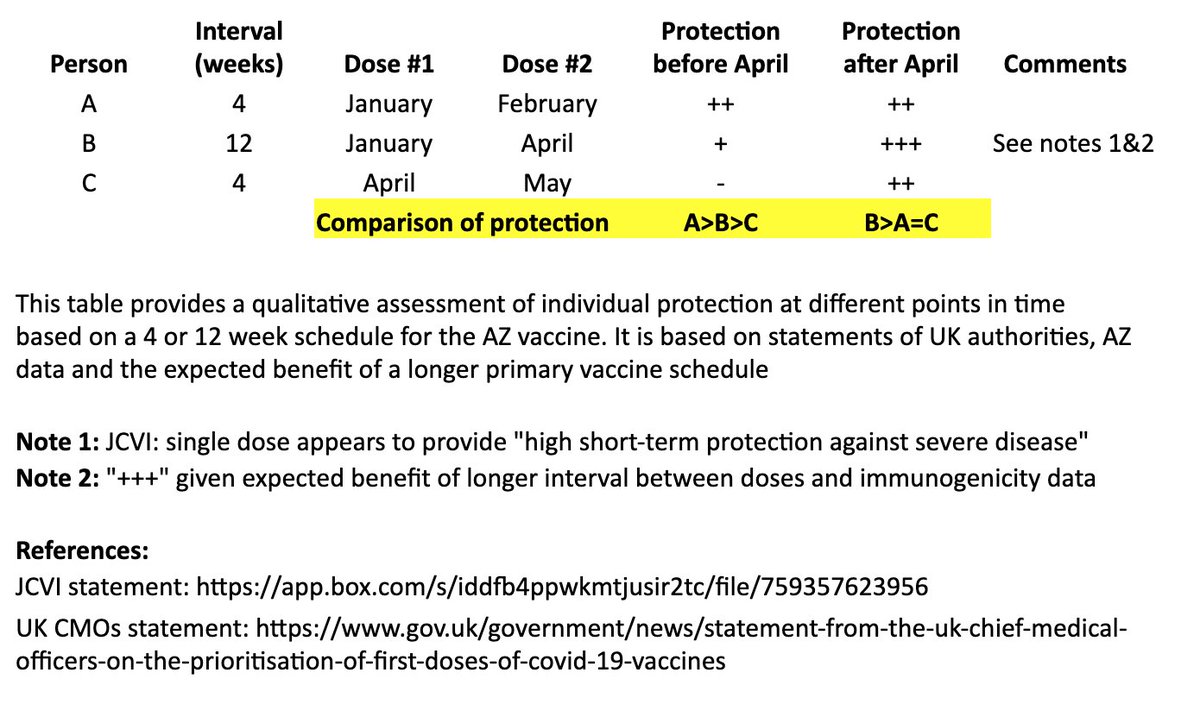
I created a simple table to illustrate the individual impact of the "flexible second dose timing" now recommended in the UK.
Coincidentally, @bob_wachter & @ashishkjha just tackled the US policy question in this important piece. 1/
https://t.co/n5bHkdIo0c
In @washingtonpost, @ashishkjha & I argue for the 2nd-shot-deferred strategy, partly by invoking the Mike Tyson principle. https://t.co/ZxrgVj3TJe We both came to this view because of the slow rollout & the new variant. But it's a tough call and reasonable people will disagree.
— Bob Wachter (@Bob_Wachter) January 3, 2021
I based this on recent statements from the UK chief medical officers, JCVI, and what we know from prior vaccine development. 2/
JCVI: https://t.co/6FQ25d6MFE
UK Chief Medical Officer (CMO) statement: https://t.co/RTpAIqgE1i
CMO letter to the profession:
This table and thread focuses on the AZ vaccine, where more data on a delayed second dose is available than with the Pfizer vaccine. It is not intended to address questions about single-dose regimens or mix & match approaches. 3/
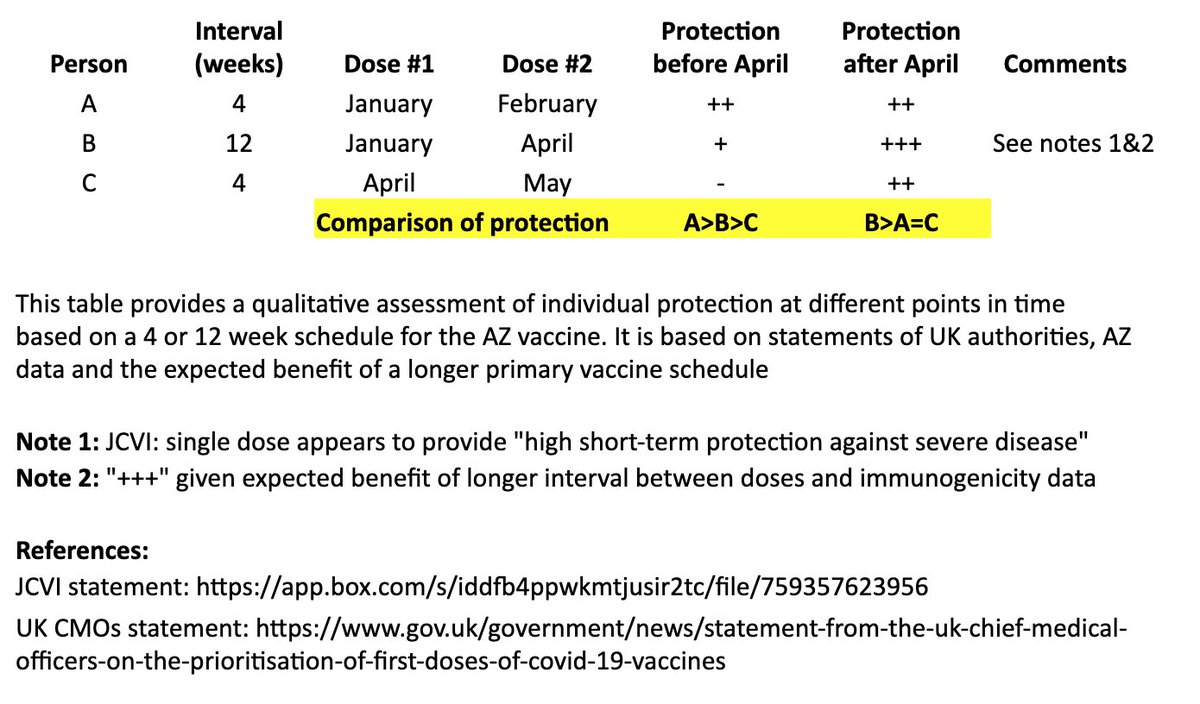
In the table, persons “A” and “B” both receive their first dose in January. “A” receives their second dose in February (4 weeks later), and “B” receives their second dose in April (12 weeks later). “C” receives their first dose in April and second dose in May (4 weeks later). 4/
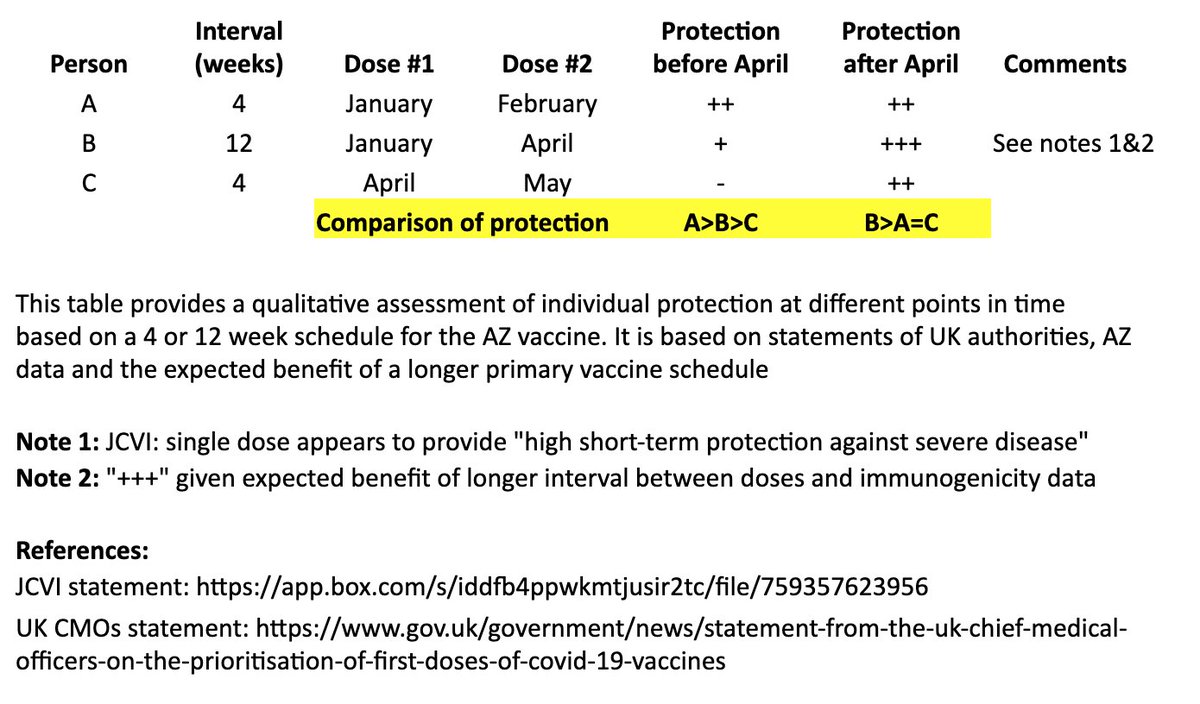
I made a qualitative comparison the potential efficacy during the two months between “A” and “B’s” second dose, as well as the potential longer-term efficacy after “B” receives their second dose. 5/
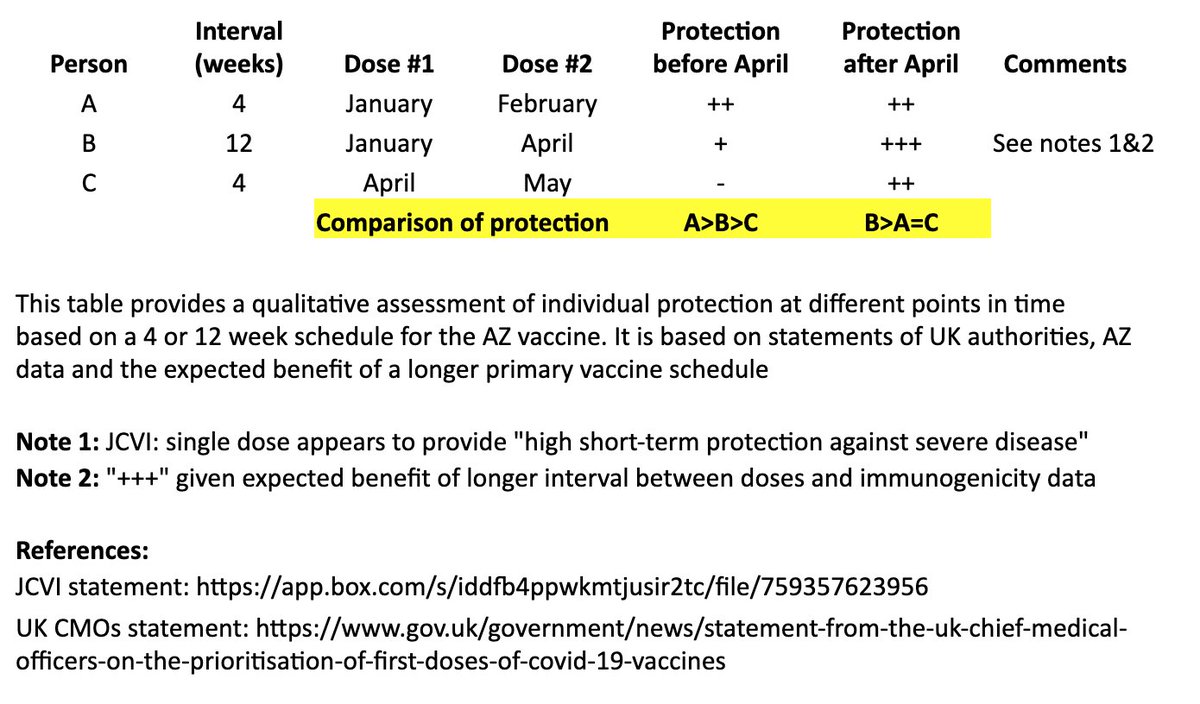









https://t.co/8amD9PQhfO
So overwhelmed. Filmed in A Cardiff Hospital (disclaimer. Not by me!) . Notice the empty beds also. \U0001f92c\U0001f92c pic.twitter.com/dZcE9cMERy
— Tracy make the world great \U0001f4ab (@TracyICQ) December 30, 2020
https://t.co/pmCsSJ6a1p
Romford Hospital - my man on the ground was there for over an hour. pic.twitter.com/jk0BxtLF5o
— Ministry Of Dissent, #EndTheLockdown #KBF (@MinistryDissent) December 30, 2020
https://t.co/KRPpFVCSgz
Don\u2019t know who this is or when it was filmed, but it raises questions #NightingaleHospitals pic.twitter.com/eyuIZuJGDz
— R Bemath (@RBemath) December 29, 2020
https://t.co/9iyvqPyo9O
Worth noting on hospital occupancy. I\u2019m hearing anecdotal evidence of same from whistleblowers in hospitals including in London. https://t.co/fahC18EbEw
— Richard Tice (@TiceRichard) December 29, 2020

Have you tried Botox for Migraine? Did it help? https://t.co/a29gDd65mT
— Migraine Again (@MigraineAgain) December 30, 2020
Way to discern spastic unilateral Superior trapezius muscle: look in mirror, view your auto driver license photo, & to pinch leading edge of each Superior trapezius to determine which leading edge is painful to pressure & also thicker; from supporting a chronically tilted head.
Looking in the mirror enables the person to view which shoulder is lower. The head usually tilts toward the lower shoulder side; causing Superior trapezius muscle on the higher shoulder side to be spastic from chronically supporting a tilted head (weighs about 10#).
The drivers license photo often confirms which shoulder is lower and provides clue as to which direction the head usually & chronically tilts. Some people pick a posed posture & straighten up when they pose for a photo. Therefore, other and more candid photos might be examined.
Often, especially in hyper-mobile women, the spine is curved with a functional scoliosis (straightens when reclined), and this is explanation for the asymmetric shoulders and tilted head.

