
Also, scientists stand apart from their subject matter--as distantly as possible. Physicians, on the contrary, are in "a relationship" with patients. 2/
Sorry, Dr. Jha, but you shouldn't confuse medical care with the scientific enterprise. Although the 2 are commonly conflated, they are really distinct. 1/
The hearings are meant as a questioning of the scientific process
— Ashish K. Jha, MD, MPH (@ashishkjha) December 7, 2020
To sew doubt on what we know and how we know it
So a group of us organized a response, which we just posted on our website
It isn't pro or anti hydroxy
Its about the scientific method and why it matters
2/3
Also, scientists stand apart from their subject matter--as distantly as possible. Physicians, on the contrary, are in "a relationship" with patients. 2/
First, scientific knowledge is often limited or provisional, especially with a new disease.
Second, for every patient there are myriad circumstances that influence a medical decision. /3
Fourth--and most pertinent here--one cannot narrowly limit the scientific knowledge to only RCTs as you do in your statement. /4
I won't rehash all the arguments here (and there are many!) but I'm sure you're familiar with this piece by Dr. Frieden from only a couple of years ago https://t.co/f7jHvDujUZ /5
My point is that your attacks miss the point: Medical standards cannot be reduced to scientific ones. /12
If you have an interest in the historical background for this, here are a couple of the pieces that I wrote on this topic a few years ago: /14
https://t.co/q5ECfaN47b
More from Science










Epic thread incoming:
I'm going to answer the question so many people have been asking this week:
WHAT IS PROJECT X???
Here's the definitive thread to tell you - and show you -precisely what Project X is
Grab a drink, sit down with me and let's #TalkLiberation
<3
1/?
"Project X" is actually called "PanQuake".
Pan means "all". Quake is the huge effect our voices can have when our communications are uncensored and when we have access to brand new functionality that *enhances* our social reach, rather than diminishes it
Here's our logo:
2/?

You can follow the fledgling official PanQuake Twitter account here: @pan_quake and see our super cool new website here: https://t.co/F7wLSeM6aK
You can find our donation page here: https://t.co/VICFnsR0RX
Keep reading this thread to find out why we created it & what it is
3/?
SPOILER ALERT: Much of the content below this point is from my personal slides & speech notes from today's launch event. That stream got totally ruined by (big) tech problems, but I'm happy to report everything is turning out wonderfully
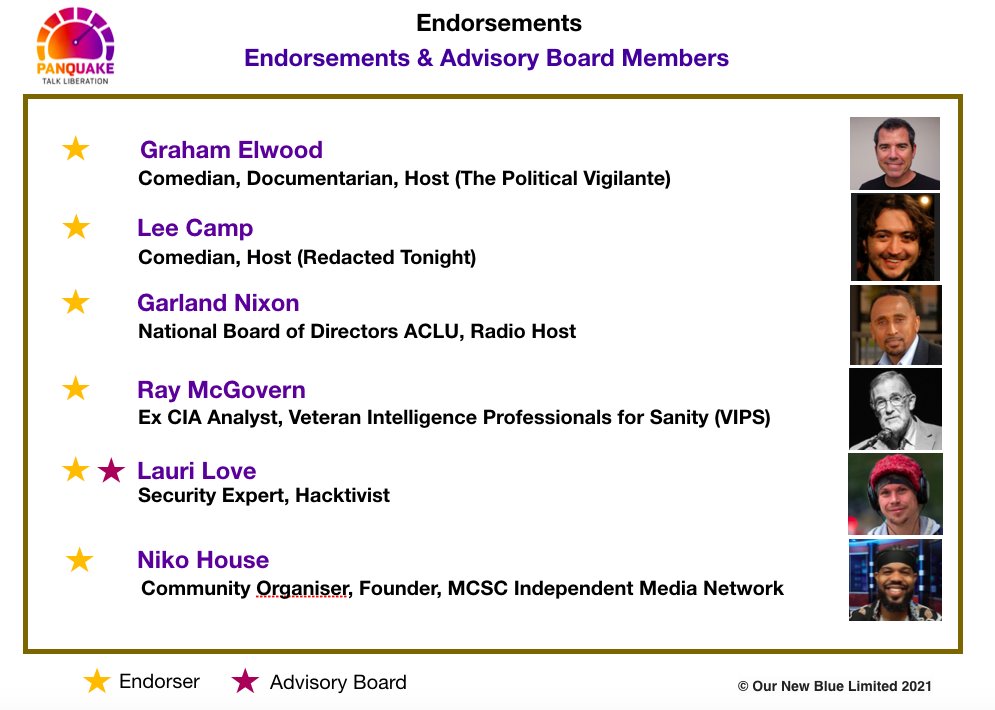
Here are some of our most high profile & dedicated public advocates for PanQuake - many of whom were scheduled to appear at our launch. All of whom stuck around for hours, to do a prerecord of the event, which is being edited, processed & uploaded for you as I write this.
5/?
I'm going to answer the question so many people have been asking this week:
WHAT IS PROJECT X???
Here's the definitive thread to tell you - and show you -precisely what Project X is
Grab a drink, sit down with me and let's #TalkLiberation
<3
1/?
"Project X" is actually called "PanQuake".
Pan means "all". Quake is the huge effect our voices can have when our communications are uncensored and when we have access to brand new functionality that *enhances* our social reach, rather than diminishes it
Here's our logo:
2/?
You can follow the fledgling official PanQuake Twitter account here: @pan_quake and see our super cool new website here: https://t.co/F7wLSeM6aK
You can find our donation page here: https://t.co/VICFnsR0RX
Keep reading this thread to find out why we created it & what it is
3/?
SPOILER ALERT: Much of the content below this point is from my personal slides & speech notes from today's launch event. That stream got totally ruined by (big) tech problems, but I'm happy to report everything is turning out wonderfully
Not one single team member or guest left. We are all still here, smiling not crying, as we record this event and will get it out to you all very soon :)
— Suzie Dawson (@Suzi3D) January 17, 2021
I'm so proud of everyone, what an amazing crewhttps://t.co/RmE0BicIXF
Here are some of our most high profile & dedicated public advocates for PanQuake - many of whom were scheduled to appear at our launch. All of whom stuck around for hours, to do a prerecord of the event, which is being edited, processed & uploaded for you as I write this.
5/?

You May Also Like





Great article from @AsheSchow. I lived thru the 'Satanic Panic' of the 1980's/early 1990's asking myself "Has eveyrbody lost their GODDAMN MINDS?!"
The 3 big things that made the 1980's/early 1990's surreal for me.
1) Satanic Panic - satanism in the day cares ahhhh!
2) "Repressed memory" syndrome
3) Facilitated Communication [FC]
All 3 led to massive abuse.
"Therapists" -and I use the term to describe these quacks loosely - would hypnotize people & convince they they were 'reliving' past memories of Mom & Dad killing babies in Satanic rituals in the basement while they were growing up.
Other 'therapists' would badger kids until they invented stories about watching alligators eat babies dropped into a lake from a hot air balloon. Kids would deny anything happened for hours until the therapist 'broke through' and 'found' the 'truth'.
FC was a movement that started with the claim severely handicapped individuals were able to 'type' legible sentences & communicate if a 'helper' guided their hands over a keyboard.
For three years I have wanted to write an article on moral panics. I have collected anecdotes and similarities between today\u2019s moral panic and those of the past - particularly the Satanic Panic of the 80s.
— Ashe Schow (@AsheSchow) September 29, 2018
This is my finished product: https://t.co/otcM1uuUDk
The 3 big things that made the 1980's/early 1990's surreal for me.
1) Satanic Panic - satanism in the day cares ahhhh!
2) "Repressed memory" syndrome
3) Facilitated Communication [FC]
All 3 led to massive abuse.
"Therapists" -and I use the term to describe these quacks loosely - would hypnotize people & convince they they were 'reliving' past memories of Mom & Dad killing babies in Satanic rituals in the basement while they were growing up.
Other 'therapists' would badger kids until they invented stories about watching alligators eat babies dropped into a lake from a hot air balloon. Kids would deny anything happened for hours until the therapist 'broke through' and 'found' the 'truth'.
FC was a movement that started with the claim severely handicapped individuals were able to 'type' legible sentences & communicate if a 'helper' guided their hands over a keyboard.

https://t.co/6cRR2B3jBE
Viruses and other pathogens are often studied as stand-alone entities, despite that, in nature, they mostly live in multispecies associations called biofilms—both externally and within the host.
https://t.co/FBfXhUrH5d

Microorganisms in biofilms are enclosed by an extracellular matrix that confers protection and improves survival. Previous studies have shown that viruses can secondarily colonize preexisting biofilms, and viral biofilms have also been described.

...we raise the perspective that CoVs can persistently infect bats due to their association with biofilm structures. This phenomenon potentially provides an optimal environment for nonpathogenic & well-adapted viruses to interact with the host, as well as for viral recombination.

Biofilms can also enhance virion viability in extracellular environments, such as on fomites and in aquatic sediments, allowing viral persistence and dissemination.

Viruses and other pathogens are often studied as stand-alone entities, despite that, in nature, they mostly live in multispecies associations called biofilms—both externally and within the host.
https://t.co/FBfXhUrH5d
Microorganisms in biofilms are enclosed by an extracellular matrix that confers protection and improves survival. Previous studies have shown that viruses can secondarily colonize preexisting biofilms, and viral biofilms have also been described.
...we raise the perspective that CoVs can persistently infect bats due to their association with biofilm structures. This phenomenon potentially provides an optimal environment for nonpathogenic & well-adapted viruses to interact with the host, as well as for viral recombination.
Biofilms can also enhance virion viability in extracellular environments, such as on fomites and in aquatic sediments, allowing viral persistence and dissemination.