
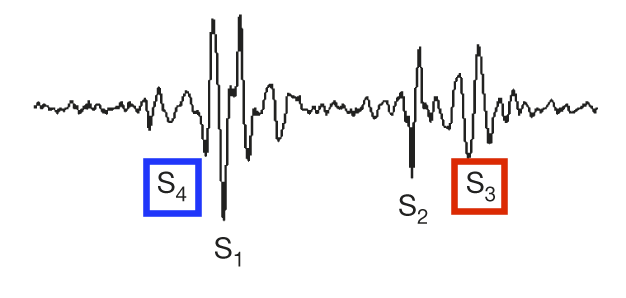
Q: Why do we use a stethoscope?
A: For many reasons, and here’s one of them that I will argue is undervalued. And is still at the heart (hint hint) of some ongoing research…
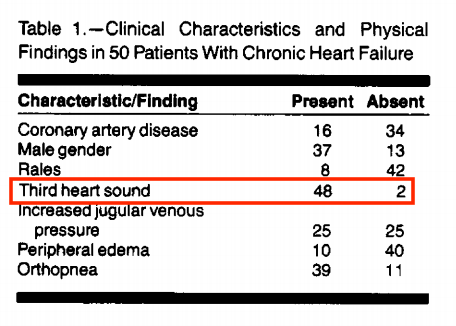
This cohort had quite the notable med regimen: digoxin (84%), furosemide (84%), vasodilators (56%), and milrinone (4%); 39/50 were being evaluated for transplant
A plausible explanation for this observation in chronic (as opposed to acute HF):

https://t.co/UKT9XDf0mc


https://t.co/xWeIhzZ93b



https://t.co/Plaev6fe4q
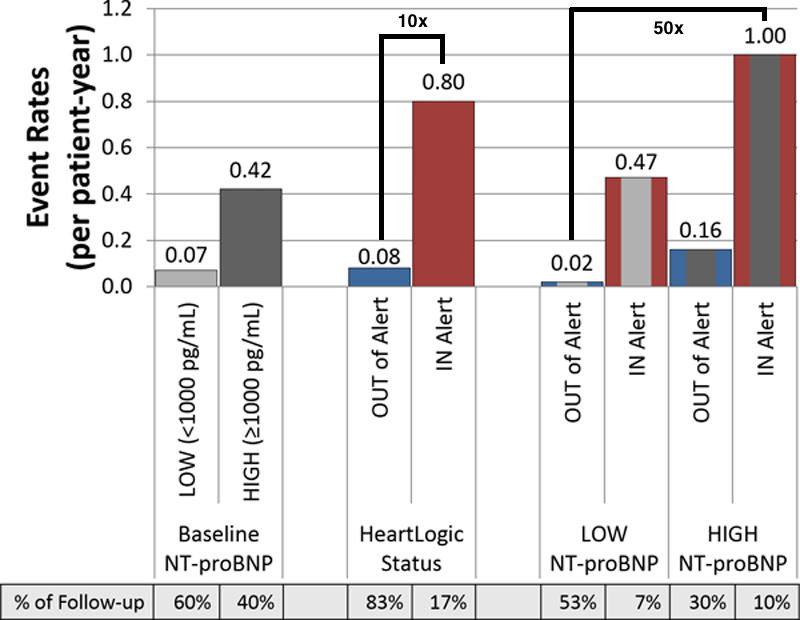
Substratification showed that the lowest risk group (low NT-proBNP and not in alert status) vs. the highest risk group (high NT-proBNP levels and being in alert status), had a 50-fold increased risk of an HF event (1.00/pt-year vs 0.02/pt-year).
Look how far we’ve come from simply placing a stethoscope on a patient - although this is still not obsolete, it has led to some excellent advances over the years.
https://t.co/6jyS3lhfE5
Next exciting thing on the agenda @PennStHershey - using @nanowearinc\u2019s wearable vest with nano-fiber ECG pads and a very sensitive microphone to quantify S3 heart sounds in the inaudible range, to predict HF exacerbations. pic.twitter.com/kmxpRL6a0Y
— Alexander Hajduczok, MD (@AHajduczok) December 19, 2020
Ali, O., Hajduczok, A.G. & Boehmer, J.P. Remote Physiologic Monitoring for Heart Failure. Curr Cardiol Rep 22, 68 (2020).
https://t.co/1bmFVDU4Ij
More from Health


I think @SamAdlerBell in his quest to be the contrarian on Fauci gets several things wrong here. 1/
First, the failure last year actually was driven by the White House, the #Trump inner circle. Watch what's happening now, the US' scientific and public health infrastructure is creaking back to life. 2/
I think Sam underestimates the decimation of many of our health agencies over the past four years and the establishment of ideological control over them during the pandemic. 3/
I also am puzzled why Tony gets the blame for not speaking up, etc. Robert Redfield, Brett Giroir, Deb Birx, Jerome Adams, Alex Azar all could have done the same. 4/
Several of these people Bob Redfield, Brett Giroir, Alex Azar were led by craven ambition, Jerome Adams by cowardice, but I do think Deb Birx and Tony tried as institutionalists, insiders to make a difference. 5/
— Matthew Yglesias (@mattyglesias) January 30, 2021
First, the failure last year actually was driven by the White House, the #Trump inner circle. Watch what's happening now, the US' scientific and public health infrastructure is creaking back to life. 2/
I think Sam underestimates the decimation of many of our health agencies over the past four years and the establishment of ideological control over them during the pandemic. 3/
I also am puzzled why Tony gets the blame for not speaking up, etc. Robert Redfield, Brett Giroir, Deb Birx, Jerome Adams, Alex Azar all could have done the same. 4/
Several of these people Bob Redfield, Brett Giroir, Alex Azar were led by craven ambition, Jerome Adams by cowardice, but I do think Deb Birx and Tony tried as institutionalists, insiders to make a difference. 5/





You May Also Like



Master Thread of all my threads!
Hello!! 👋
• I have curated some of the best tweets from the best traders we know of.
• Making one master thread and will keep posting all my threads under this.
• Go through this for super learning/value totally free of cost! 😃
1. 7 FREE OPTION TRADING COURSES FOR
2. THE ABSOLUTE BEST 15 SCANNERS EXPERTS ARE USING
Got these scanners from the following accounts:
1. @Pathik_Trader
2. @sanjufunda
3. @sanstocktrader
4. @SouravSenguptaI
5. @Rishikesh_ADX
3. 12 TRADING SETUPS which experts are using.
These setups I found from the following 4 accounts:
1. @Pathik_Trader
2. @sourabhsiso19
3. @ITRADE191
4.
4. Curated tweets on HOW TO SELL STRADDLES.
Everything covered in this thread.
1. Management
2. How to initiate
3. When to exit straddles
4. Examples
5. Videos on
Hello!! 👋
• I have curated some of the best tweets from the best traders we know of.
• Making one master thread and will keep posting all my threads under this.
• Go through this for super learning/value totally free of cost! 😃
1. 7 FREE OPTION TRADING COURSES FOR
A THREAD:
— Aditya Todmal (@AdityaTodmal) November 28, 2020
7 FREE OPTION TRADING COURSES FOR BEGINNERS.
Been getting lot of dm's from people telling me they want to learn option trading and need some recommendations.
Here I'm listing the resources every beginner should go through to shorten their learning curve.
(1/10)
2. THE ABSOLUTE BEST 15 SCANNERS EXPERTS ARE USING
Got these scanners from the following accounts:
1. @Pathik_Trader
2. @sanjufunda
3. @sanstocktrader
4. @SouravSenguptaI
5. @Rishikesh_ADX
The absolute best 15 scanners which experts are using.
— Aditya Todmal (@AdityaTodmal) January 29, 2021
Got these scanners from the following accounts:
1. @Pathik_Trader
2. @sanjufunda
3. @sanstocktrader
4. @SouravSenguptaI
5. @Rishikesh_ADX
Share for the benefit of everyone.
3. 12 TRADING SETUPS which experts are using.
These setups I found from the following 4 accounts:
1. @Pathik_Trader
2. @sourabhsiso19
3. @ITRADE191
4.
12 TRADING SETUPS which experts are using.
— Aditya Todmal (@AdityaTodmal) February 7, 2021
These setups I found from the following 4 accounts:
1. @Pathik_Trader
2. @sourabhsiso19
3. @ITRADE191
4. @DillikiBiili
Share for the benefit of everyone.
4. Curated tweets on HOW TO SELL STRADDLES.
Everything covered in this thread.
1. Management
2. How to initiate
3. When to exit straddles
4. Examples
5. Videos on
Curated tweets on How to Sell Straddles
— Aditya Todmal (@AdityaTodmal) February 21, 2021
Everything covered in this thread.
1. Management
2. How to initiate
3. When to exit straddles
4. Examples
5. Videos on Straddles
Share if you find this knowledgeable for the benefit of others.

