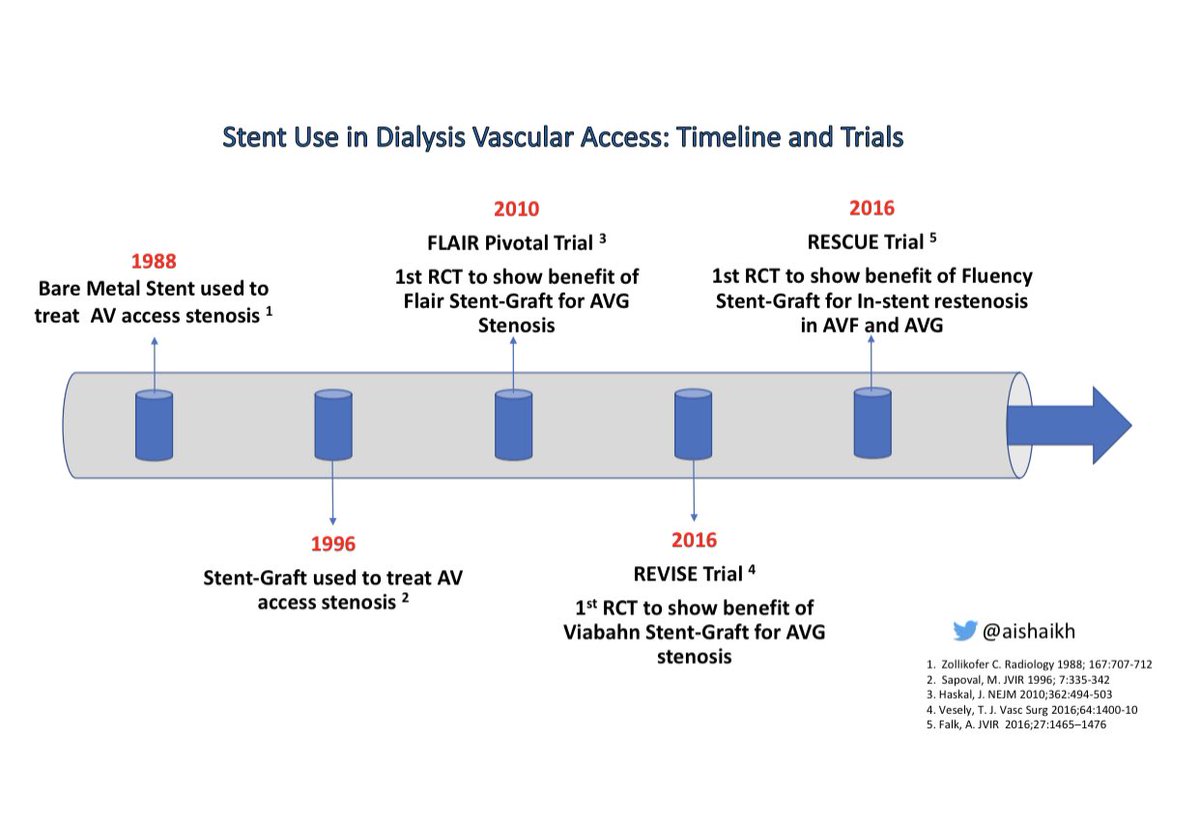
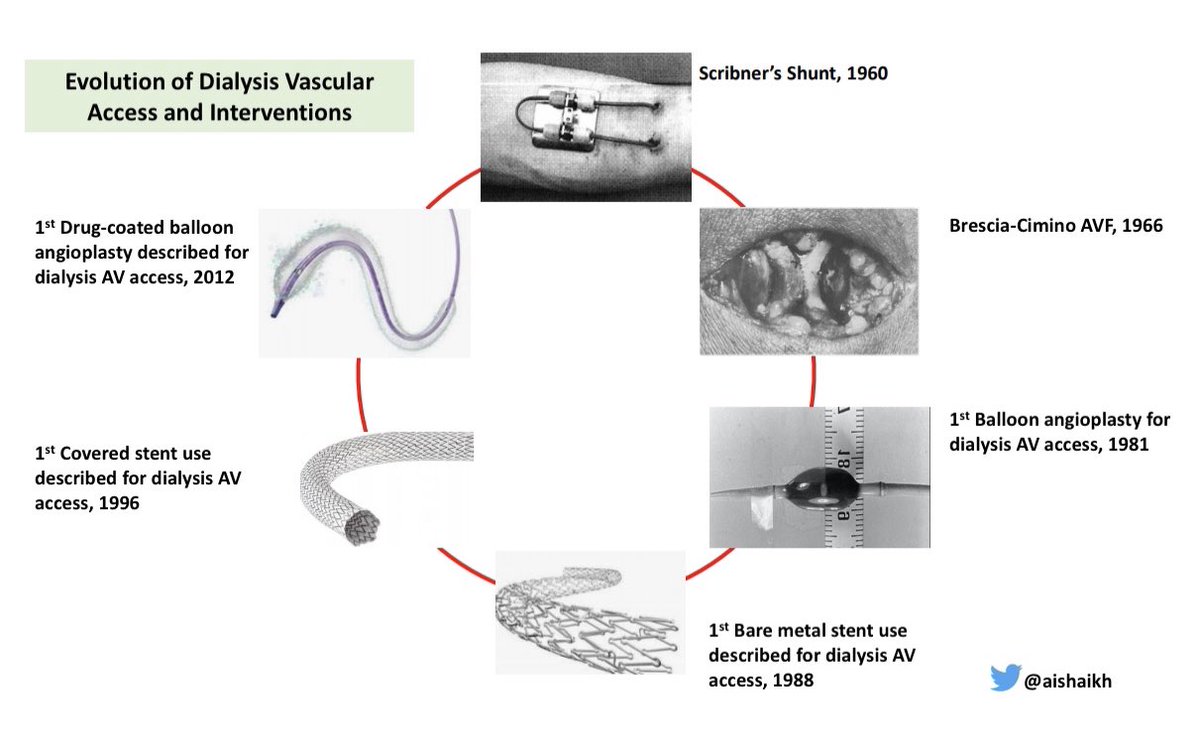
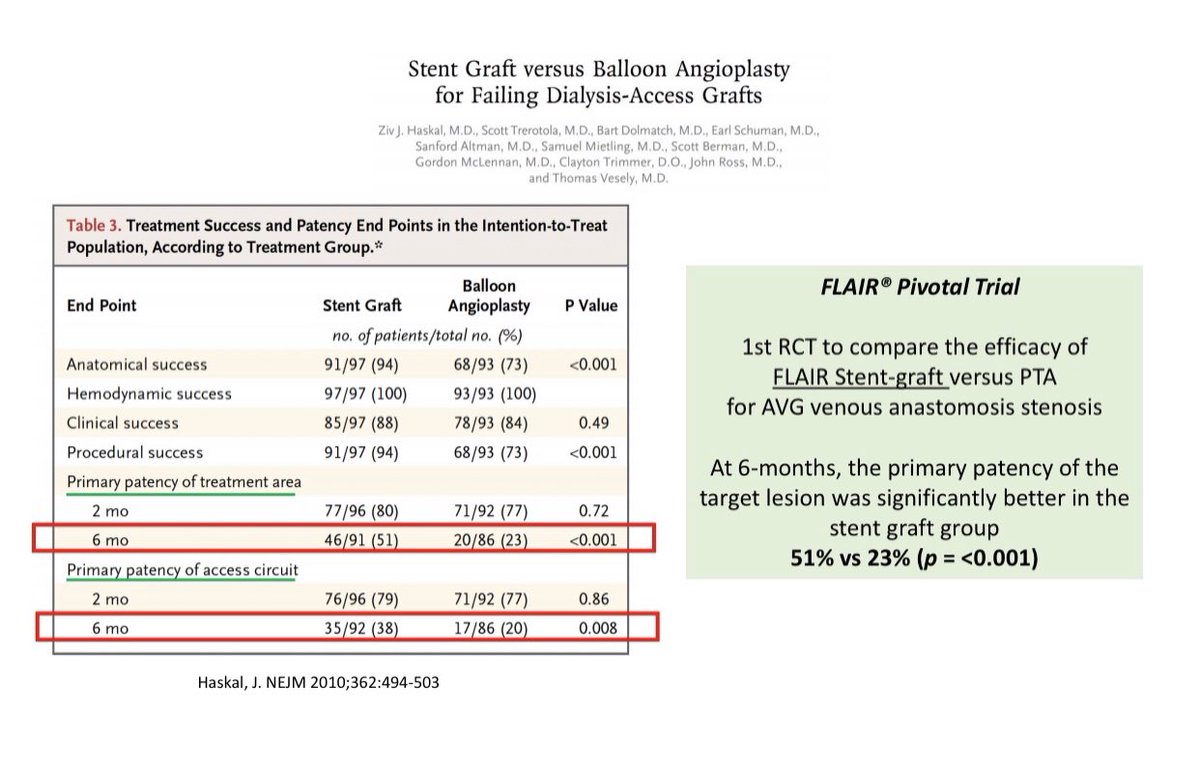
causes significant morbidity & mortality in patients on hemodialysis
⚡️Most AV access associated complications are due to vascular stenosis👇🏽
2/

In our new paper out today, autistic adults held a \u201cget to know you\u201d conversation with an unfamiliar autistic or typically-developing (TD) person. We were curious: would social interaction outcomes differ when their partner was also autistic? THREAD https://t.co/4koqUKV9G1
— Noah Sasson (@Noahsasson) December 11, 2019
How well does social cognition predict functional and social skills in autism? Our new paper attempts to answer this question. This thread summarizes why we conducted the study, what we found, and why I think it\u2019s important. https://t.co/KB1nIpK0M2
— Noah Sasson (@Noahsasson) August 16, 2019
New by @kmdebrabander and our lab: Autistic adults don\u2019t differ from non-autistic adults in the accuracy of their self-assessment on general cognitive tasks but are less accurate on social cognitive tasks. This however was unrelated to social functioning https://t.co/0MrqMKKO0r
— Noah Sasson (@Noahsasson) September 20, 2020
Ironies of Luck https://t.co/5BPWGbAxFi
— Morgan Housel (@morganhousel) March 14, 2018
"Luck is the flip side of risk. They are mirrored cousins, driven by the same thing: You are one person in a 7 billion player game, and the accidental impact of other people\u2019s actions can be more consequential than your own."
4/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
...indication, first of all that testing for a (single) respiratory virus is done outside of surveillance systems or need for specific therapy, but even so the lack of consideration of Ct, symptoms and clinical findings when interpreting its result. https://t.co/gHH6kwRdZG
6/10
— Dr. Thomas Binder, MD (@Thomas_Binder) October 22, 2020
The neither validated nor standardised hypersensitive RT-PCR test / Ct 35-45 for SARS-CoV-2 is abused to mislabel (also) other diseases, especially influenza, as COVID-19.https://t.co/AkFIfTCTkS
External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results.https://t.co/mbNY8bdw1p pic.twitter.com/OQBD4grMth
— Dr. Thomas Binder, MD (@Thomas_Binder) November 29, 2020
Thread web\u2b06\ufe0f\u2b07\ufe0f
— Dr. Thomas Binder, MD (@Thomas_Binder) December 16, 2020
The fabrication of the "asymptomatic (super) spreader" is the coronation of the total nons(ci)ense in the belief system of #CoronasWitnesses.
Asymptomatic transmission 0.7%; 95% CI 0%-4.9% - could well be 0%!https://t.co/VeZTzxXfvT
8/8
— Dr. Thomas Binder, MD (@Thomas_Binder) March 24, 2020
By the way, who the f*** created this obviously (almost) worldwide definition of #CoronaDeath?
This is not only medical malpractice, this is utterly insane!https://t.co/FFsTx4L2mw