
Heartburn can be caused by acid reflux or gastroesophageal reflux disease (GERD).
STOMACH ULCERS
A CASE TODAY
Stomach ulcers are sores in the lining of the stomach or small intestine. They occur when the protective mucus that lines the stomach becomes ineffective.
Symptoms
The classic symptom of a stomach ulcer is indigestion, also called dyspepsia.
Heartburn can be caused by acid reflux or gastroesophageal reflux disease (GERD).
It is worth noting that not all stomach ulcers cause indigestion.
Stomach ulcer symptoms tend to be more distinct than heartburn, but symptoms can still be vague.
weight loss
nausea and vomiting
not eating because of pain
burping
bloating
pain may be relieved by eating, drinking, or taking antacids
Diet
Dietary changes can help prevent stomach ulcers from developing.
People at risk of stomach ulcers should include more of the following nutrients in their diet:
Fiber: Diets high in soluble dietary fiber reduce the risk of developing stomach ulcers.
Selenium: This may reduce the risk of infection complications and may also promote healing.
Avoiding alcohol and caffeine can also help reduce the risk, as they both cause the body to produce more gastric acid. This can lead to stomach ulcers.
Causes
The two main causes of ulcers of the stomach and small intestine are:
a class of painkillers called nonsteroidal anti-inflammatory drugs (NSAIDs)
Less common causes of stomach ulcers include:
Zollinger-Ellison syndrome: This is a rare disease that causes an excess of stomach acid to be produced.
Certain behaviors and factors increase the chances of developing a stomach ulcer.
These include:
smoking
overproducing calcium, or hypercalcemia
genetics
consuming alcohol frequently
Stomach ulcers are more common in individuals over 50 years of age. People can develop a stomach ulcer at any age, but they are much less common in children.
NSAID drugs and stomach ulcers
A group of painkillers known as NSAIDs carries a risk of stomach ulcers. The two best-known NSAIDs are aspirin and ibuprofen.
Stronger NSAIDs, such as those that need a prescription, are riskier for stomach ulcers than those that can be bought over-the-counter (OTC).
Types
Stomach ulcers are one type of peptic ulcers.
Treatment
If the doctor thinks there is a stomach ulcer, they may try to remove the cause by:
trying the "test-and-treat" approach if the cause is thought to be H. pylori bacteria
H2-receptor antagonists, which prevent the stomach from producing excess acid
antacids or alginate. These are available to purchase over-the-counter.
Symptoms often subside quickly following treatment. However, the treatment should be continued, especially if the ulcer is due to an H. pylori infection.
Surgical treatments
In certain cases, surgery may be an option. For instance, if the ulcer continues to return, will not heal, bleeds, or prevents food from leaving the belly
removing the ulcer
tying off bleeding blood vessels
sewing tissue from another site onto the ulcer
cutting the nerve that controls stomach acid production
Complications from stomach ulcers such as bleeding or perforation are rare.
Diagnosis
Doctors follow the symptoms of a stomach ulcer by asking questions about how the pain feels, where and when it happens, and how frequent and long-lasting it has been.
Endoscopy: A camera is inserted at the end of a long, thin, flexible tube to look at the gut lining. A biopsy may also be taken.
When to see a doctor
Anyone who thinks they may have an ulcer in their stomach should consult their doctor. Any stomach symptoms that last for more than a few days or keep happening need evaluation
A slow-bleeding ulcer can be signaled by symptoms of anemia, such as being tired and breathless. More serious bleeding is an urgent medical problem and can be signaled if blood is vomited up, or stools are black and sticky.
More from Health

this simple, counter narrative fact keeps cropping up all over the world.
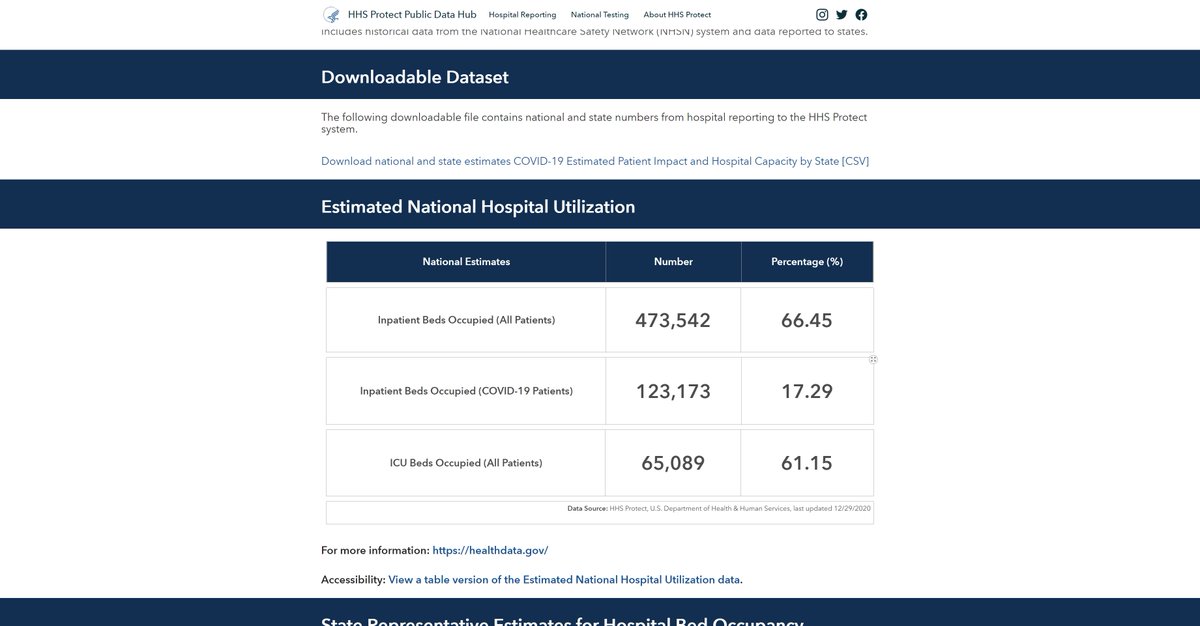
hospital and ICU utilization has been and remains low this year.
it's terribly curious that so few of these monitoring tools provide historical baselines.
getting them is like pulling teeth.
we might think of this as an oversight until you see stuff like this:
this woman was arrested for filming and sharing the fact that their are empty hospitals in the UK.
that's full blown soviet. what possible honest purpose does that
this is the action of a police state and a propaganda ministry, not a well intentioned government and a public heath agency.
"we cannot let people see the truth for fear they might base their actions on real facts" is not much of a mantra for just governance.

90% full ICU sounds scary until you realize that 90-100% full is normal in flu season.
staffed ICU beds are expensive to leave empty. it's like flying with 15% of the plane empty. hospitals don't do that.
and all US hospitals are mandated to be able to flex to 120% ICU.
the US is currently at historically low ICU utilization for this time of year.
61% is "you're all going to go out of business" territory as is 66% full hospital use.
can you blame them for mining CARES act money? they'll die without it.
hospital and ICU utilization has been and remains low this year.
it's terribly curious that so few of these monitoring tools provide historical baselines.
getting them is like pulling teeth.
It took a Freedom of Information request but @Covid19DataUK acquired 2017-2019 averages for England hospitalizations.
— Yinon Weiss (@yinonw) December 31, 2020
2020 had 18% fewer hospitalizations than prior years.
All around the world, using hospital data without context of prior years is just a fear generating lie. pic.twitter.com/DJDpqhIQuw
we might think of this as an oversight until you see stuff like this:
this woman was arrested for filming and sharing the fact that their are empty hospitals in the UK.
that's full blown soviet. what possible honest purpose does that
this is the action of a police state and a propaganda ministry, not a well intentioned government and a public heath agency.
"we cannot let people see the truth for fear they might base their actions on real facts" is not much of a mantra for just governance.
90% full ICU sounds scary until you realize that 90-100% full is normal in flu season.
staffed ICU beds are expensive to leave empty. it's like flying with 15% of the plane empty. hospitals don't do that.
and all US hospitals are mandated to be able to flex to 120% ICU.
the US is currently at historically low ICU utilization for this time of year.
61% is "you're all going to go out of business" territory as is 66% full hospital use.
can you blame them for mining CARES act money? they'll die without it.





Let's talk honestly about "informed consent."
Someone with decades of training gives someone with none advice usually packed into 1-3 mins. Huge amount is based on trust. Huge potential for bias built in. But also there is no obligation to provide real alternative options.
I am classified as 'gifted' (obnoxious and ableist term). I mention because of what I am about to say. You all know that I was an ambulatory wheelchair user previously - could stand - but contractures have ended that. When I pleaded for physio, turned down. But did you know...
I recently was chatting with a doctor I know and explaining what happened and the day the physiatrist told me it was too late and nothing could be done. The doctor asked if I'd like one of her friends/colleagues to give second opinion. I said yes please! So...
She said can you send me MRI and other imaging they did to determine it wasn't possible to address your contractures.
Me: What?
Dr.: They did a MRI first before deciding right?
Me: No
Dr: What did they do??!
Me: Examined me for 2 minutes.
Dr: I am very angry rn. Can't talk.
My point is you don't even know if you are making "informed" decisions because the only source of information you have is the person who has already decided what they think you should do. And may I remind you of a word called 'compliance.'
Someone with decades of training gives someone with none advice usually packed into 1-3 mins. Huge amount is based on trust. Huge potential for bias built in. But also there is no obligation to provide real alternative options.
MAiD isn't eugenics. The task for the medical profession is to ensure informed consent. Failures on that front should result in enforcement of the law. But Bill C-7 is the result of the existing regime imposing unnecessary, unconstitutional harms by blocked access to MAiD.
— Emmett Macfarlane (@EmmMacfarlane) February 13, 2021
I am classified as 'gifted' (obnoxious and ableist term). I mention because of what I am about to say. You all know that I was an ambulatory wheelchair user previously - could stand - but contractures have ended that. When I pleaded for physio, turned down. But did you know...
I recently was chatting with a doctor I know and explaining what happened and the day the physiatrist told me it was too late and nothing could be done. The doctor asked if I'd like one of her friends/colleagues to give second opinion. I said yes please! So...
She said can you send me MRI and other imaging they did to determine it wasn't possible to address your contractures.
Me: What?
Dr.: They did a MRI first before deciding right?
Me: No
Dr: What did they do??!
Me: Examined me for 2 minutes.
Dr: I am very angry rn. Can't talk.
My point is you don't even know if you are making "informed" decisions because the only source of information you have is the person who has already decided what they think you should do. And may I remind you of a word called 'compliance.'










