
Seeing a lot of this circulating on the right, so let me explain why folks are worried even though it is not literally true that every ICU bed in the country is occupied at the moment.
it's disappointing to see that we are back in the "media scare stories about hospitals" stage.
— el gato malo (@boriquagato) December 7, 2020
the good news is that, just like last time, this is simply not the case.
they either have no idea what they are saying or are seeking to mislead.
let's look.https://t.co/eWyj2txAh6
1) Stretch existing workers to do more (potentially compromising care)
2) Recruit workers from other specialties (potentially compromising care)
2) Hire additional temporary workers
Of course, the patients also stay sick longer, which brings us to ...
That's very worrying because we might be 3 weeks from peak infections, & over a month from peak hospitalizations--falling as beds are still tied up w/Thanksgiving cases
An emergency too many people wish away by staring hard at isolated statistics & saying "I don't see a problem."
More from Health

🚨Important changes to lockdown/self-isolation regulations from 5pm
The Health Protection (Coronavirus, Restrictions) (All Tiers and Self-Isolation) (England) (Amendment) Regulations 2021
£800 'house party' FPN & police can now access track & trace data
https://t.co/k9XCpVsXhC
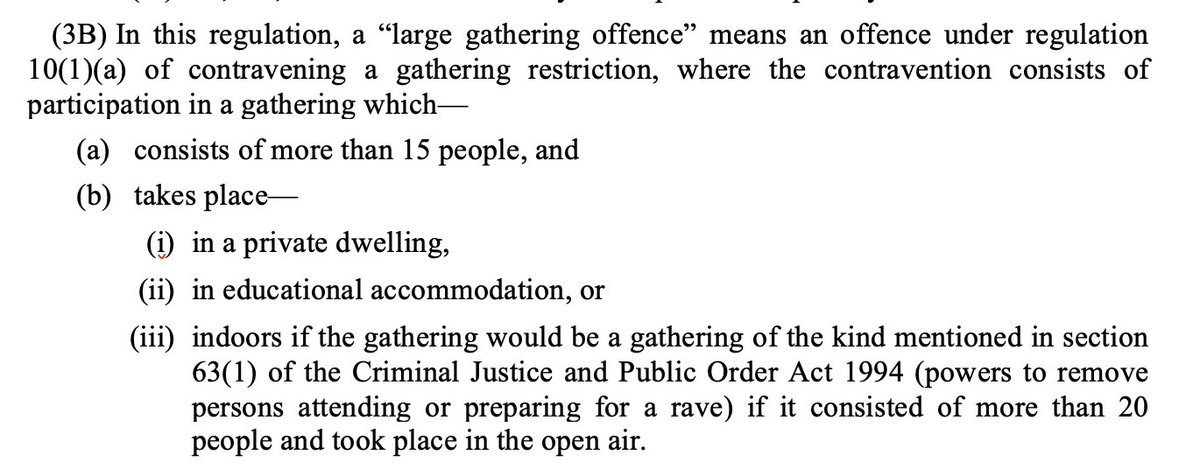
“Large gathering offence”
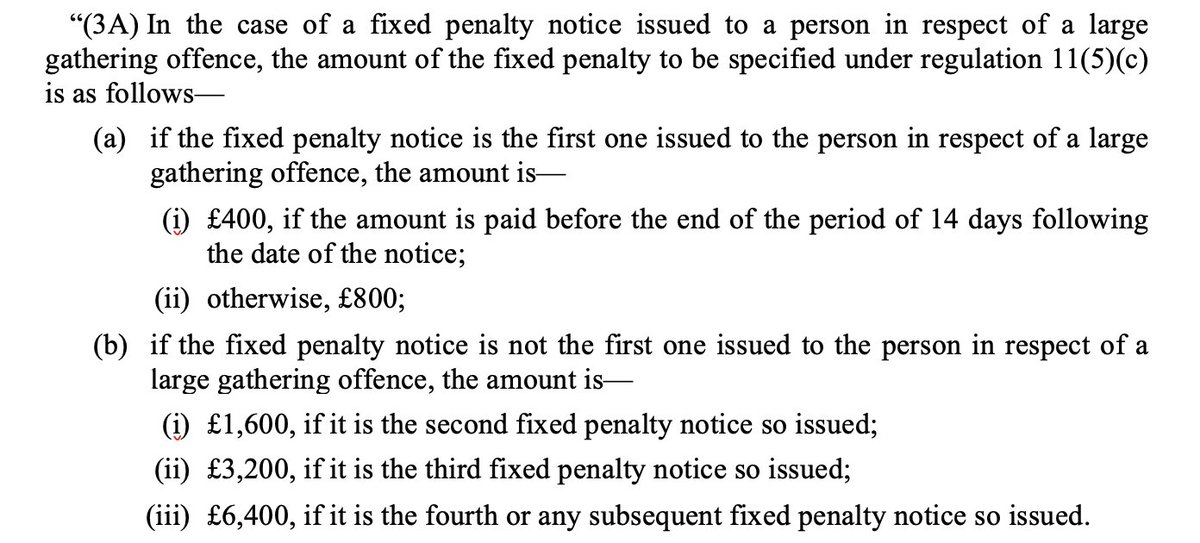
As trailed by Home Secretary last week there is now a fixed penalty notice of £800 (or £400 if you pay within 14 days) for participating in an gathering of over 15 people in a private residence
Fixed Penalty Notices double for each subsequent “large gathering offence” up to £6,400
Compare:
- Ordinary fixed penalty notice is £200 or £100 if paid in 14 days
- Holding or being involved in the holding of a gathering of over 30 people is £10,000
Second big change:
Since September has been a legal requirement to sell-isolate if you test positive/notified by Track & Trace of exposure to someone else who tested positive
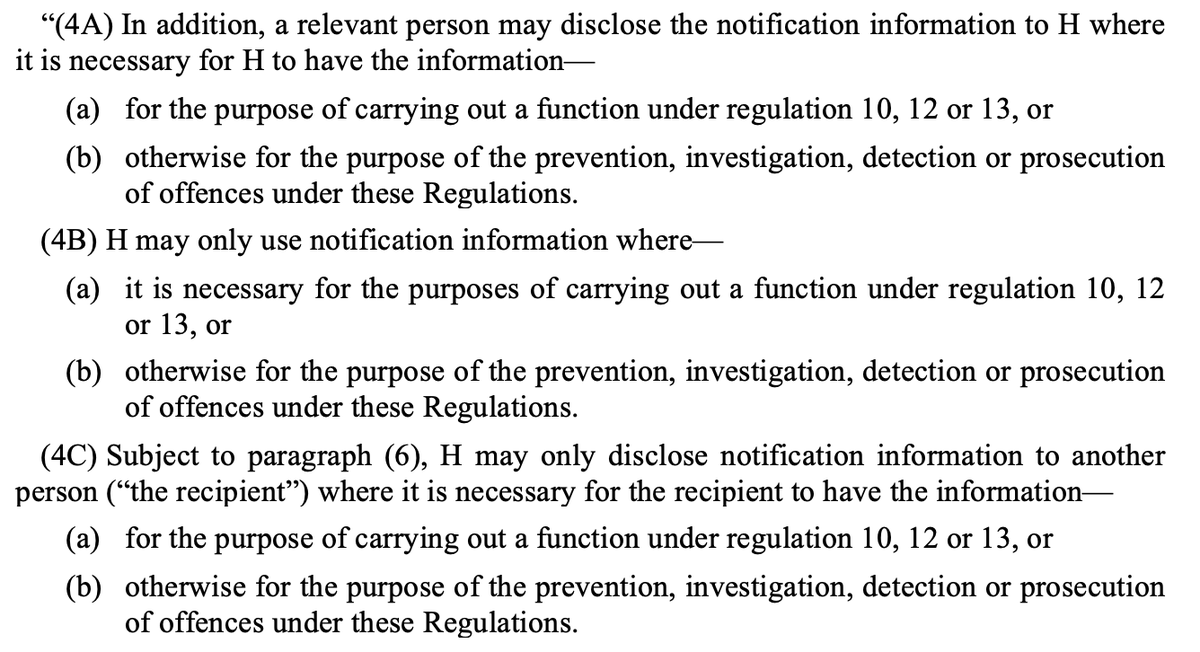
Police can now be given access to NHS Track & Trace data if for the purpose of enforcement/prosecution
This will make it easier for police to enforce people breaking self-isolation rules. Currently there has been practically no enforcement.
Data says only a small proportion of people meant to be self-isolating are fully doing so.
The Health Protection (Coronavirus, Restrictions) (All Tiers and Self-Isolation) (England) (Amendment) Regulations 2021
£800 'house party' FPN & police can now access track & trace data
https://t.co/k9XCpVsXhC
“Large gathering offence”
As trailed by Home Secretary last week there is now a fixed penalty notice of £800 (or £400 if you pay within 14 days) for participating in an gathering of over 15 people in a private residence
Fixed Penalty Notices double for each subsequent “large gathering offence” up to £6,400
Compare:
- Ordinary fixed penalty notice is £200 or £100 if paid in 14 days
- Holding or being involved in the holding of a gathering of over 30 people is £10,000
Second big change:
Since September has been a legal requirement to sell-isolate if you test positive/notified by Track & Trace of exposure to someone else who tested positive
Police can now be given access to NHS Track & Trace data if for the purpose of enforcement/prosecution
This will make it easier for police to enforce people breaking self-isolation rules. Currently there has been practically no enforcement.
Data says only a small proportion of people meant to be self-isolating are fully doing so.
Very important that obvious failures with Track and Trace and self-isolation (study late last year said 18% of people complying https://t.co/dhJUZ7Pm0l) are not painted as an enforcement issue. Plainly not. Would just pass buck to police who have almost no capacity to enforce https://t.co/Eb4Kl5Ze0E
— Adam Wagner (@AdamWagner1) January 25, 2021

1/16
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
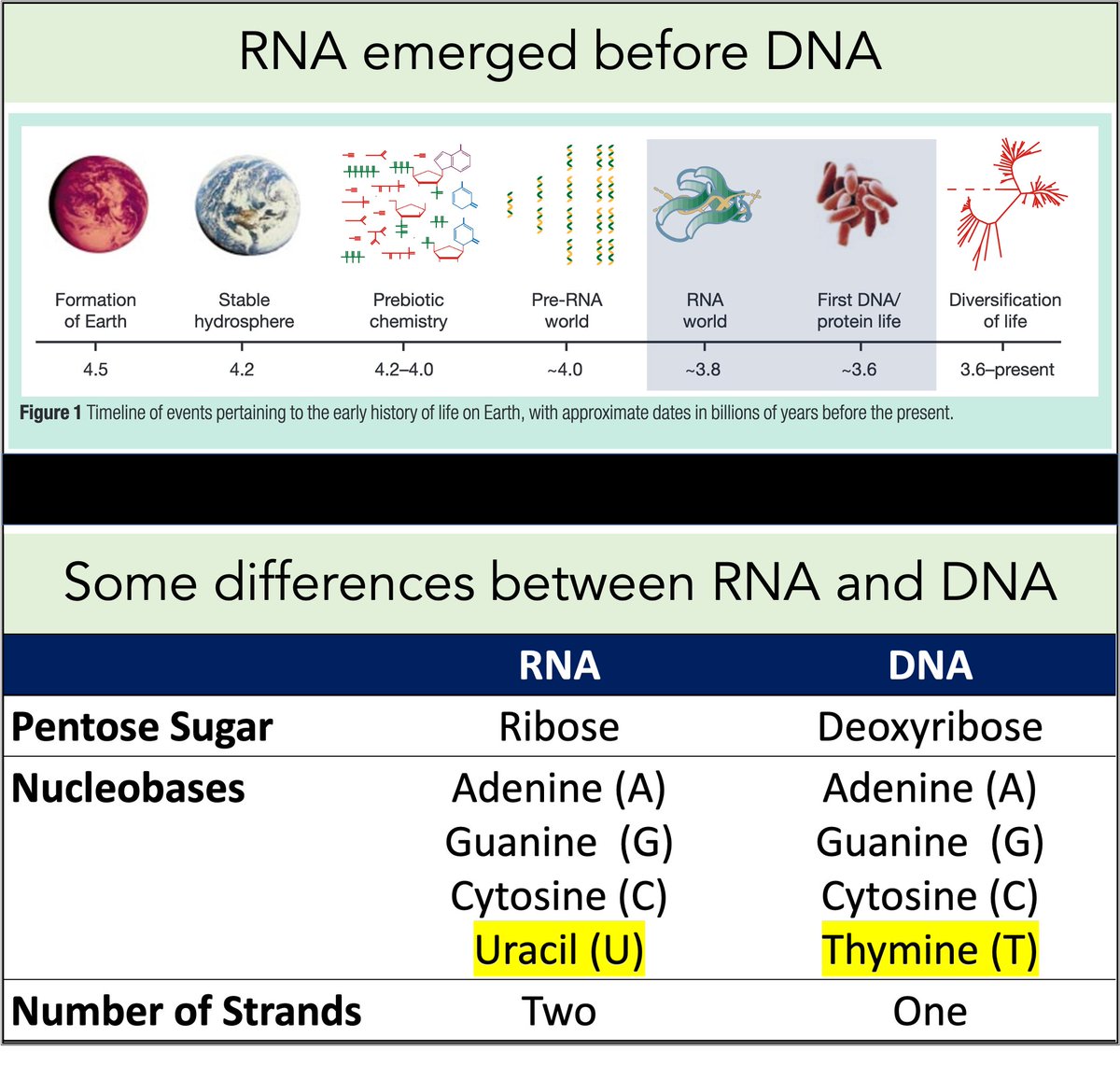
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
https://t.co/XlxT6cLLXg
3/
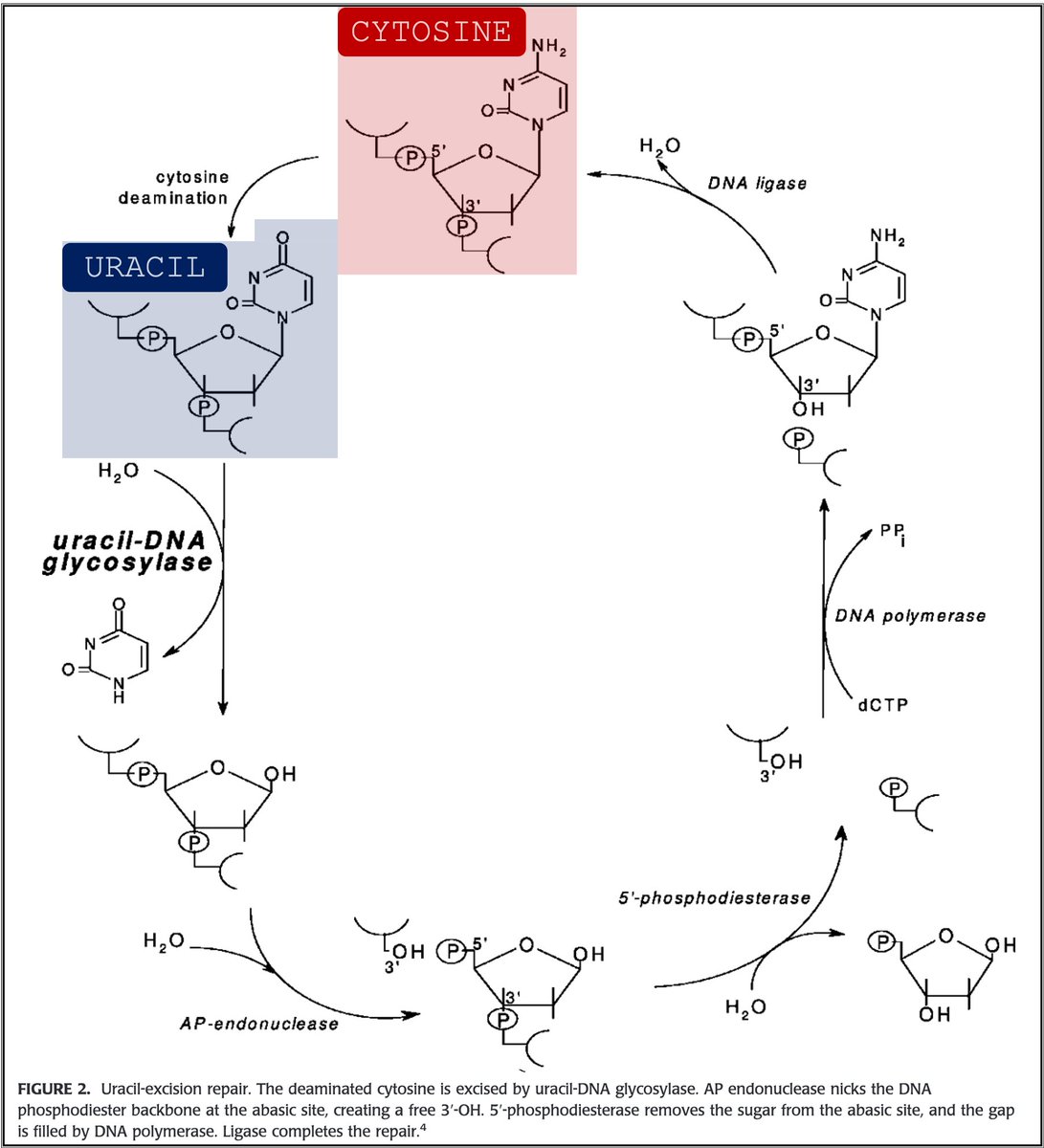
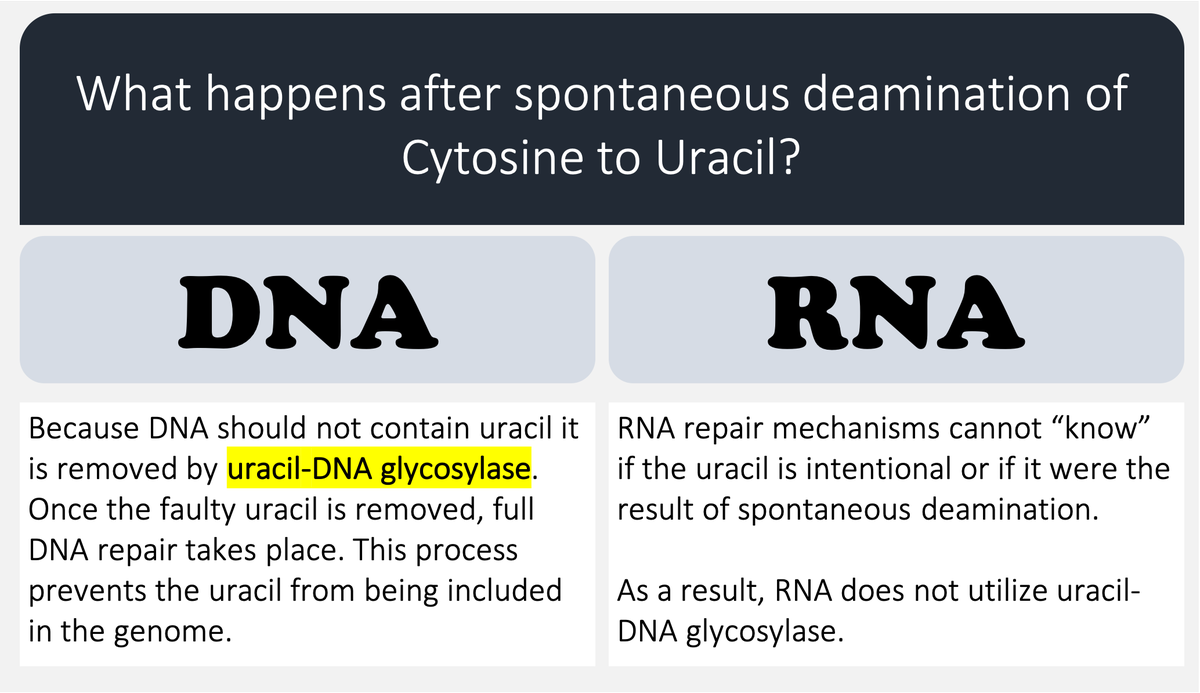
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
https://t.co/bIZGviHBUc
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
https://t.co/bIZGviHBUc
5/
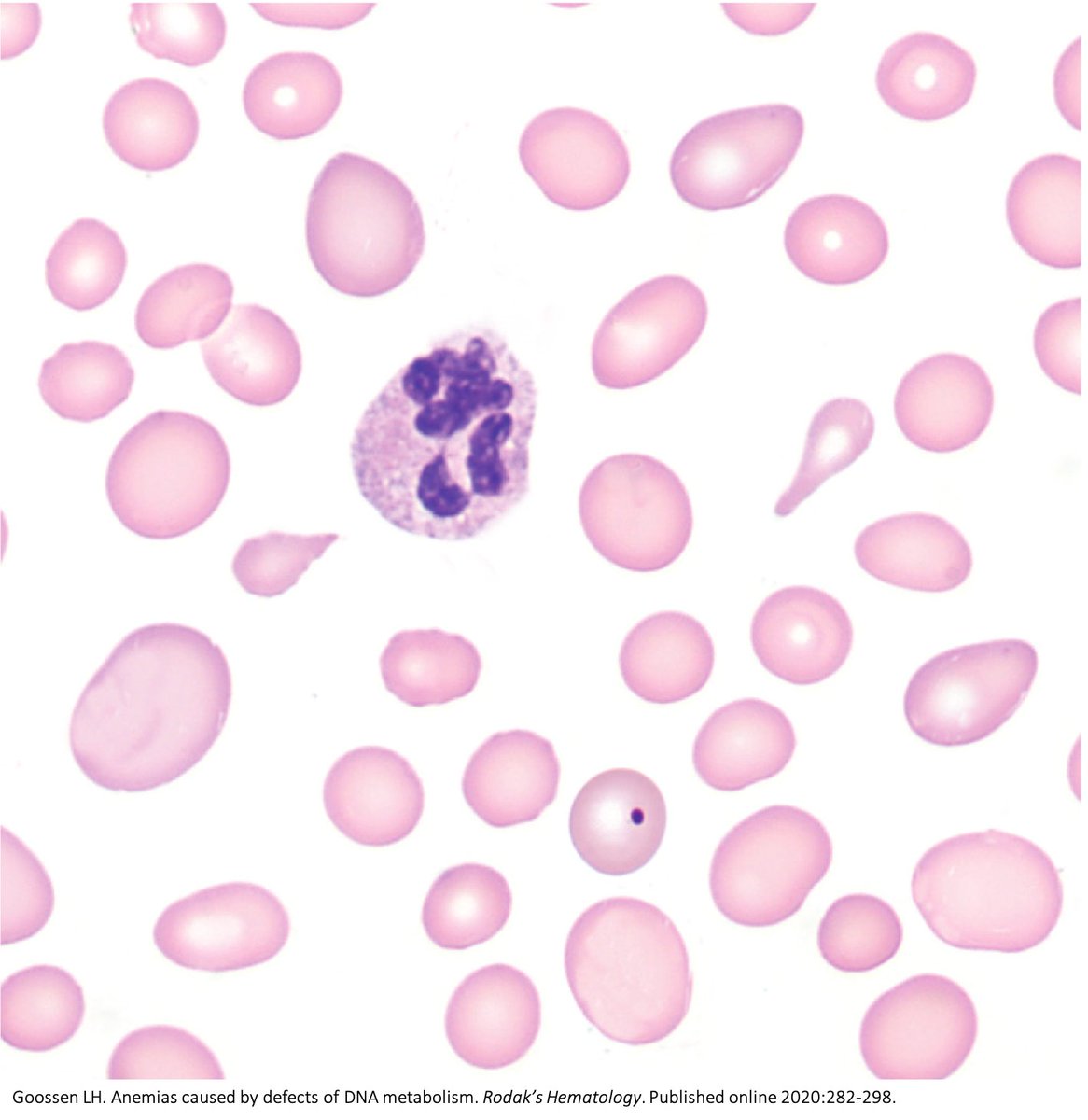
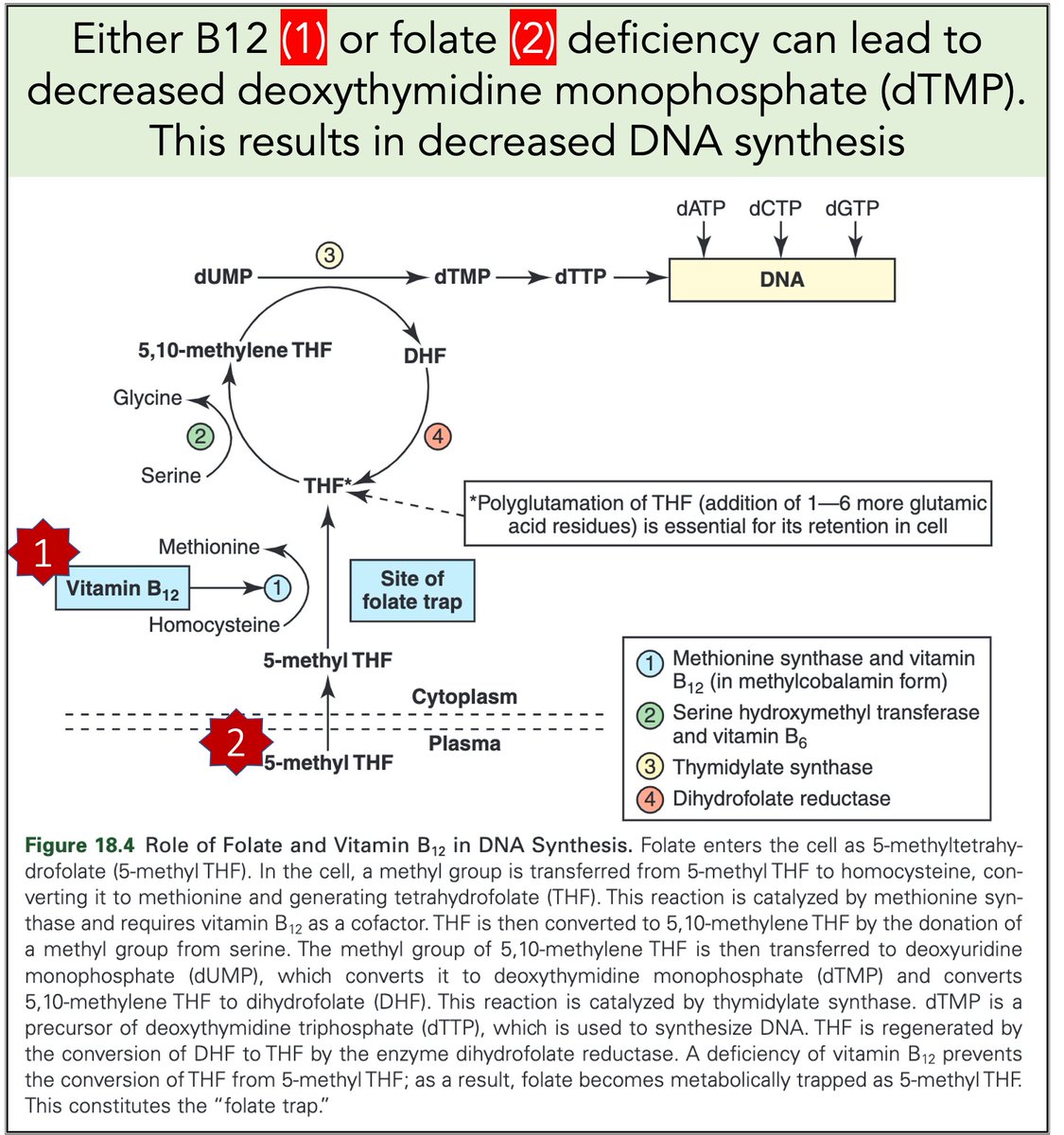
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
https://t.co/AnDUtKkbZh
Why do B12 and folate deficiencies lead to HUGE red blood cells?
And, if the issue is DNA synthesis, why are red blood cells (which don't have DNA) the key cell line affected?
For answers, we'll have to go back a few billion years.
2/
RNA came first. Then, ~3-4 billion years ago, DNA emerged.
Among their differences:
🔹RNA contains uracil
🔹DNA contains thymine
But why does DNA contains thymine (T) instead of uracil (U)?
https://t.co/XlxT6cLLXg
3/
🔑Cytosine (C) can undergo spontaneous deamination to uracil (U).
In the RNA world, this meant that U could appear intensionally or unintentionally. This is clearly problematic. How can you repair RNA when you can't tell if something is an error?
https://t.co/bIZGviHBUc
4/
DNA's use of T instead of U means that spontaneous C → U deamination can be corrected without worry that an intentional U is being removed.
DNA requires greater stability than RNA so the transition to a thymine-based structure was beneficial.
https://t.co/bIZGviHBUc
5/
Let's return to megaloblastic anemia secondary to B12 or folate deficiency.
When either is severely deficient deoxythymidine monophosphate (dTMP*) production is hindered. With less dTMP, DNA synthesis is abnormal.
[*Note: thymine is the base in dTMP]
https://t.co/AnDUtKkbZh





![Peter McCormack [Jan/3\u279e\u20bf \U0001f511\u220e]](https://pbs.twimg.com/profile_images/1524287442307723265/_59ITDbJ_normal.jpg)



