
We struggle to staff many of those beds fully with 100,000 NHS post unfilled inc 1 in 8 in nursing
A short thread about hospital bed pressures
This may surprise some people outside the healthcare bubble but for a population of c 60 million, England (pre-pandemic) only had just over 100,000 General and Acute Hospital Beds and c 4,300 ICU beds and both running close to full
We struggle to staff many of those beds fully with 100,000 NHS post unfilled inc 1 in 8 in nursing
This takes further beds out of availability
Meanwhile, infection control measures mean hospitals taking beds out of bays to keep beds further apart and care activities can take longer with all the PPE and precautions meaning staff under further time pressure
A hall in an exhibition centre with beds is NOT a hospital. They are not staffed for the volume of patients they could notionally take and only 3 of the 7/8 have taken any in patients (totalling less than 400 between them).
You May Also Like


BREAKING: @CommonsCMS @DamianCollins just released previously sealed #Six4Three @Facebook documents:
Some random interesting tidbits:
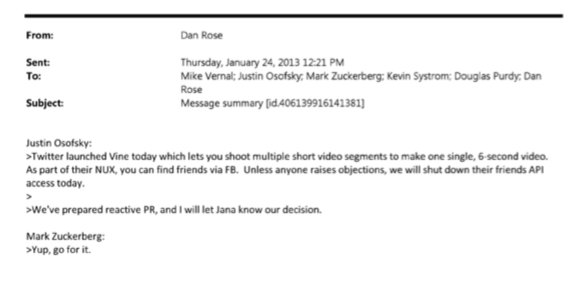
1) Zuck approves shutting down platform API access for Twitter's when Vine is released #competition
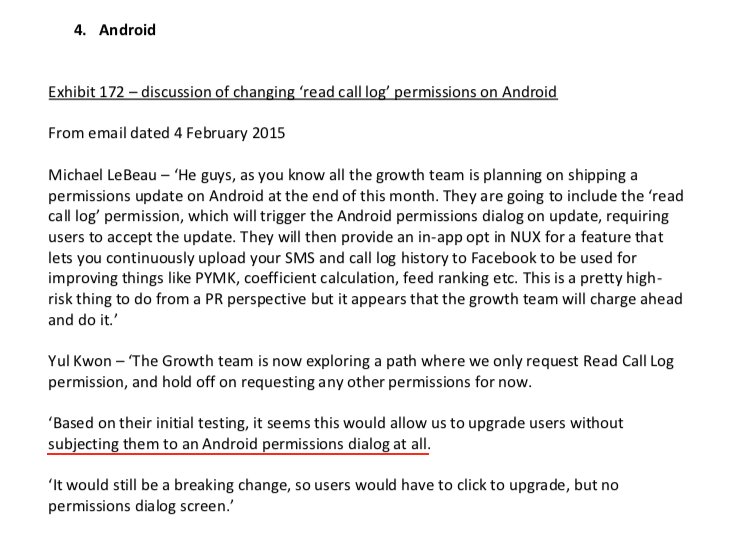
2) Facebook engineered ways to access user's call history w/o alerting users:
Team considered access to call history considered 'high PR risk' but 'growth team will charge ahead'. @Facebook created upgrade path to access data w/o subjecting users to Android permissions dialogue.
3) The above also confirms @kashhill and other's suspicion that call history was used to improve PYMK (People You May Know) suggestions and newsfeed rankings.
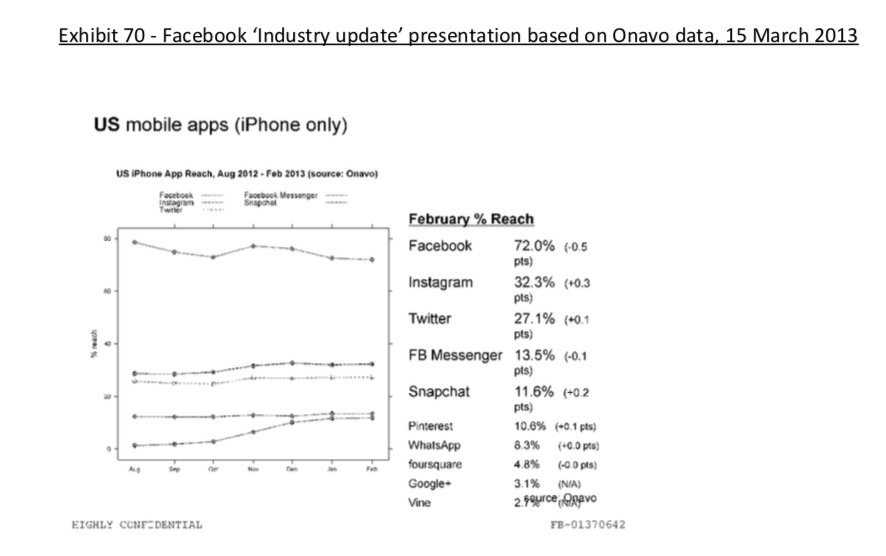
4) Docs also shed more light into @dseetharaman's story on @Facebook monitoring users' @Onavo VPN activity to determine what competitors to mimic or acquire in 2013.
https://t.co/PwiRIL3v9x
Some random interesting tidbits:
1) Zuck approves shutting down platform API access for Twitter's when Vine is released #competition
2) Facebook engineered ways to access user's call history w/o alerting users:
Team considered access to call history considered 'high PR risk' but 'growth team will charge ahead'. @Facebook created upgrade path to access data w/o subjecting users to Android permissions dialogue.
3) The above also confirms @kashhill and other's suspicion that call history was used to improve PYMK (People You May Know) suggestions and newsfeed rankings.
4) Docs also shed more light into @dseetharaman's story on @Facebook monitoring users' @Onavo VPN activity to determine what competitors to mimic or acquire in 2013.
https://t.co/PwiRIL3v9x









