As someone who has studied healthcare handoffs for a while, I can’t stop thinking about the Presidential one coming up. I see I’m not the only one. But this is not like any handoff. My nerdy 🧵 #MedTwitter #Inauguration2021
More from Health




I applaud the #EUCancerPlan *BUT* caution: putting #meat 🥩 (a nourishing, evolutionary food) in the same box as 🚬 to solve a contemporary health challenge, would be basing policy on assumptions rather than robust data.
#FollowTheScience yes, but not just part of it!
THREAD👇
1/ Granted, some studies have pointed to ASSOCIATIONS of HIGH intake of red & processed meats with (slightly!) increased colorectal cancer incidence. Also, @WHO/IARC is often mentioned in support (usually hyperbolically so).
But, let’s have a closer look at all this! 🔍

2/ First, meat being “associated” with cancer is very different from stating that meat CAUSES cancer.
Unwarranted use of causal language is widespread in nutritional sciences, posing a systemic problem & undermining credibility.
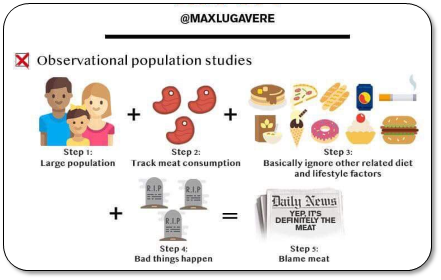
3/ That’s because observational data are CONFOUNDED (even after statistical adjustment).
Healthy user bias is a major problem. Healthy middle classes are TOLD to eat less red meat (due to historical rather than rational reasons, cf link). So, they
4/ What’s captured here is sociology, not physiology.
Health-focused Westerners eat less red meat, whereas those who don’t adhere to dietary advice tend to have unhealthier lifestyles.
That tells us very little about meat AS SUCH being responsible for disease.
#FollowTheScience yes, but not just part of it!
THREAD👇
\U0001f534LIVE \U0001f4c5Today \u23f012:00 CET
— EU_HEALTH - #EUCancerPlan (@EU_Health) February 3, 2021
We are presenting today the #EUCancerPlan as part of a strong \U0001f1ea\U0001f1fa#HealthUnion
Follow the presentation live here: https://t.co/Cr8ATvzNkg#WorldCancerDay pic.twitter.com/zdByuklWV6
1/ Granted, some studies have pointed to ASSOCIATIONS of HIGH intake of red & processed meats with (slightly!) increased colorectal cancer incidence. Also, @WHO/IARC is often mentioned in support (usually hyperbolically so).
But, let’s have a closer look at all this! 🔍
2/ First, meat being “associated” with cancer is very different from stating that meat CAUSES cancer.
Unwarranted use of causal language is widespread in nutritional sciences, posing a systemic problem & undermining credibility.
3/ That’s because observational data are CONFOUNDED (even after statistical adjustment).
Healthy user bias is a major problem. Healthy middle classes are TOLD to eat less red meat (due to historical rather than rational reasons, cf link). So, they
4/ What’s captured here is sociology, not physiology.
Health-focused Westerners eat less red meat, whereas those who don’t adhere to dietary advice tend to have unhealthier lifestyles.
That tells us very little about meat AS SUCH being responsible for disease.

No-regret #hydrogen:
Charting early steps for H₂ infrastructure in Europe.
👉Summary of conclusions of a new study by @AgoraEW @AFRY_global @Ma_Deutsch @gnievchenko (1/17)
https://t.co/YA50FA57Em
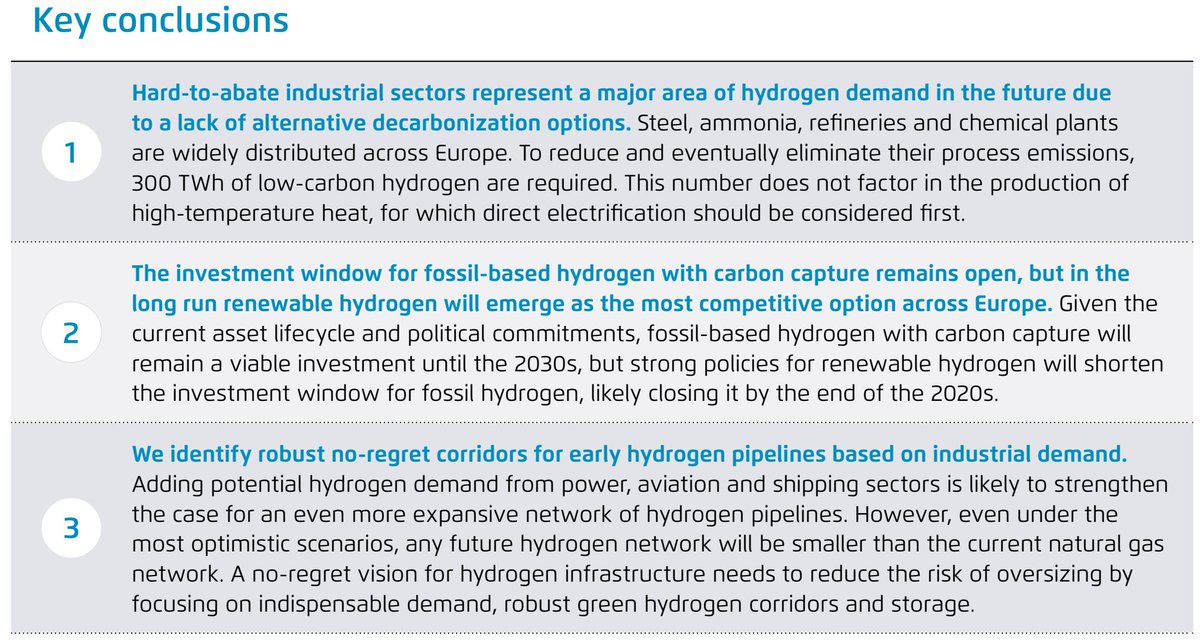
The idea behind this study is that future hydrogen demand is highly uncertain and we don’t want to spend tens of billions of euros to repurpose a network which won’t be needed. For instance, hydrogen in ground transport is a hotly debated topic https://t.co/RlnqDYVzpr (2/17)
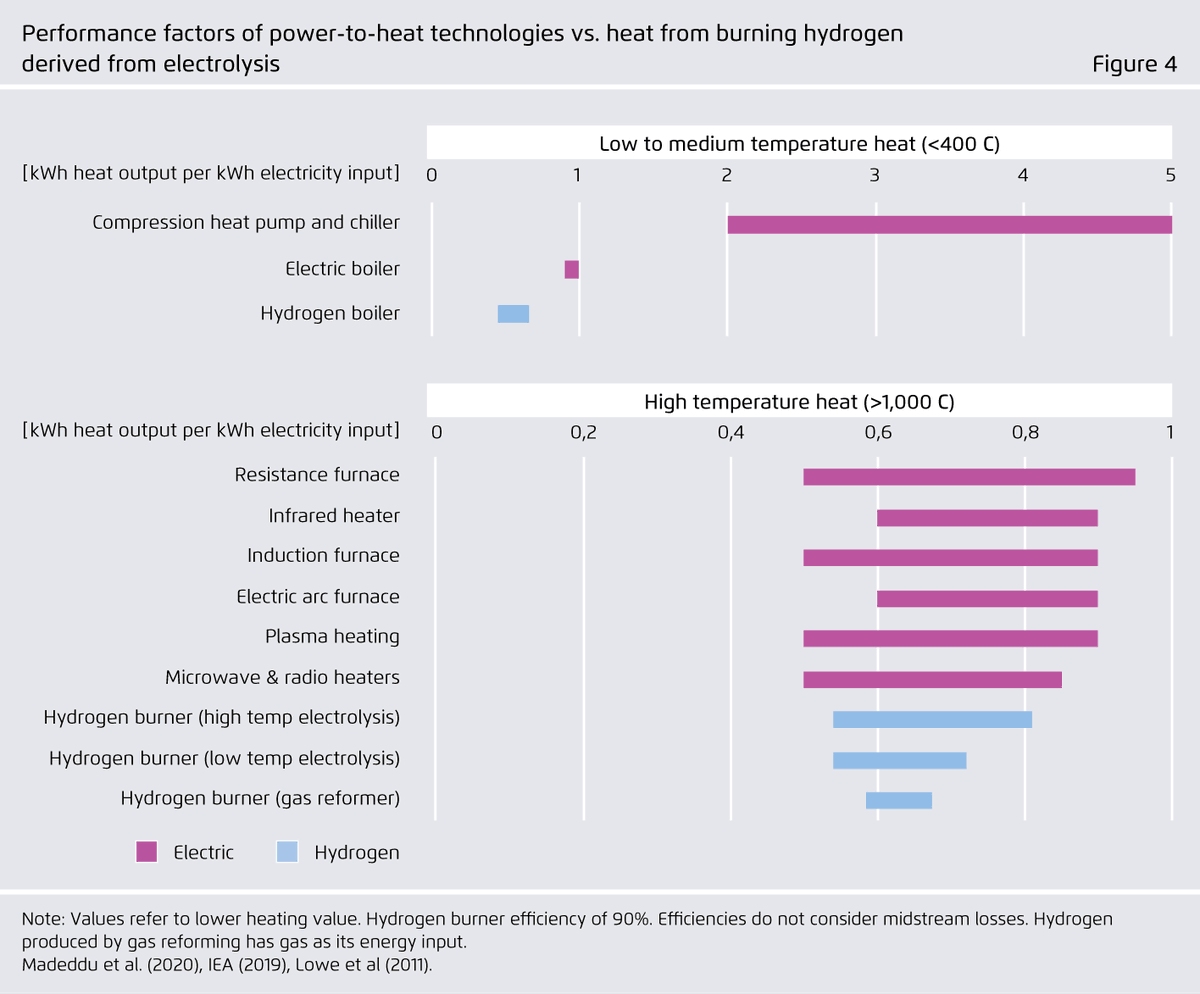
Similar things can be said about heat. 40% of today’s industrial natural gas use in the EU goes to heat below 100°C and therefore is within range of electric heat pumps – whose performance factors far exceed 100%. (3/17)

Even for higher temperatures, a range of power-to-heat (PtH) options can be more energy-efficient than hydrogen and should be considered first. Available PtH technologies can cover all temperature levels needed in industrial production (e.g. electric arc furnace: 3500°C). (4/17)
In our view, hydrogen use for feedstock and chemical reactions is the only inescapable source of industrial hydrogen demand in Europe that does not lend itself to electrification. Examples include ammonia, steel, and petrochemical industries. (5/17)
Charting early steps for H₂ infrastructure in Europe.
👉Summary of conclusions of a new study by @AgoraEW @AFRY_global @Ma_Deutsch @gnievchenko (1/17)
https://t.co/YA50FA57Em
The idea behind this study is that future hydrogen demand is highly uncertain and we don’t want to spend tens of billions of euros to repurpose a network which won’t be needed. For instance, hydrogen in ground transport is a hotly debated topic https://t.co/RlnqDYVzpr (2/17)
Similar things can be said about heat. 40% of today’s industrial natural gas use in the EU goes to heat below 100°C and therefore is within range of electric heat pumps – whose performance factors far exceed 100%. (3/17)
Even for higher temperatures, a range of power-to-heat (PtH) options can be more energy-efficient than hydrogen and should be considered first. Available PtH technologies can cover all temperature levels needed in industrial production (e.g. electric arc furnace: 3500°C). (4/17)
In our view, hydrogen use for feedstock and chemical reactions is the only inescapable source of industrial hydrogen demand in Europe that does not lend itself to electrification. Examples include ammonia, steel, and petrochemical industries. (5/17)