
As US hospitals make the necessary shuffle to accommodate the current wave, I would like to remind leadership about the study done on the psychological status of frontline hospital workers during NYC's spring Covid surge (thread).
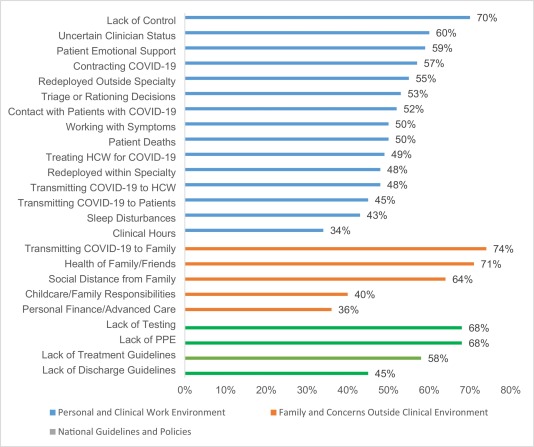
- Perceptions of a lack of control and/or uncertainty
- Performing clinical work that is outside of your specialty
- The need/expectation for healthcare providers to provide social support to patients in lieu of their families (due to visitation restrictions)
- And also fears related to getting/transmitting Covid within the work environment - in particular, the uncertain Covid status of other healthcare providers
More from Health













You May Also Like
















And here they are...
THE WINNERS OF THE 24 HOUR STARTUP CHALLENGE
Remember, this money is just fun. If you launched a product (or even attempted a launch) - you did something worth MUCH more than $1,000.
#24hrstartup
The winners 👇
#10
Lattes For Change - Skip a latte and save a life.
https://t.co/M75RAirZzs
@frantzfries built a platform where you can see how skipping your morning latte could do for the world.
A great product for a great cause.
Congrats Chris on winning $250!

#9
Instaland - Create amazing landing pages for your followers.
https://t.co/5KkveJTAsy
A team project! @bpmct and @BaileyPumfleet built a tool for social media influencers to create simple "swipe up" landing pages for followers.
Really impressive for 24 hours. Congrats!

#8
SayHenlo - Chat without distractions
https://t.co/og0B7gmkW6
Built by @DaltonEdwards, it's a platform for combatting conversation overload. This product was also coded exclusively from an iPad 😲
Dalton is a beast. I'm so excited he placed in the top 10.

#7
CoderStory - Learn to code from developers across the globe!
https://t.co/86Ay6nF4AY
Built by @jesswallaceuk, the project is focused on highlighting the experience of developers and people learning to code.
I wish this existed when I learned to code! Congrats on $250!!

THE WINNERS OF THE 24 HOUR STARTUP CHALLENGE
Remember, this money is just fun. If you launched a product (or even attempted a launch) - you did something worth MUCH more than $1,000.
#24hrstartup
The winners 👇
#10
Lattes For Change - Skip a latte and save a life.
https://t.co/M75RAirZzs
@frantzfries built a platform where you can see how skipping your morning latte could do for the world.
A great product for a great cause.
Congrats Chris on winning $250!
#9
Instaland - Create amazing landing pages for your followers.
https://t.co/5KkveJTAsy
A team project! @bpmct and @BaileyPumfleet built a tool for social media influencers to create simple "swipe up" landing pages for followers.
Really impressive for 24 hours. Congrats!
#8
SayHenlo - Chat without distractions
https://t.co/og0B7gmkW6
Built by @DaltonEdwards, it's a platform for combatting conversation overload. This product was also coded exclusively from an iPad 😲
Dalton is a beast. I'm so excited he placed in the top 10.
#7
CoderStory - Learn to code from developers across the globe!
https://t.co/86Ay6nF4AY
Built by @jesswallaceuk, the project is focused on highlighting the experience of developers and people learning to code.
I wish this existed when I learned to code! Congrats on $250!!