I am done giving this doctor or team grace. I started with "We are tremendously grateful for all you are doing." He seemed irritated to speak to us. Literally I asked, "What is the likelihood our mom will die on current support, in the next 24 hours, so we can plan travel?"
I know busy. I did 22 admissions one night while doing crosscover. I want to say "burnout" but this sounds like culture.
This team is actually making their own jobs harder. All my doctor friend conversations result in a pragmatic realism, not anxiety. I am trying to make safe decisions
More from For later read



(1/50)
#Cardano “Understanding Kamali”
#Cardano will be the underpinning of the emergence of Africa.
To grasp the full weight of the SOLUTIONS #Cardano can provide it is pertinent to read “Understanding Africa” as I will draw directly from the PROBLEMS laid out.
(2/50)
Here is a link if you have not already read
(3/50)
What I will attempt to do here, is to create an immersive world for you to be placed in to grasp the weight and size of problems from the ground level and then take a grass-roots approach at solving them using #Cardano and its technology.
(4/50)
As an investor and community member of #Cardano, this should be extremely important to you as you have a stake (pun intended) in this.
“You are paid in direct proportion to the difficulty of the problems you solve” - @elonmusk
(5/50)
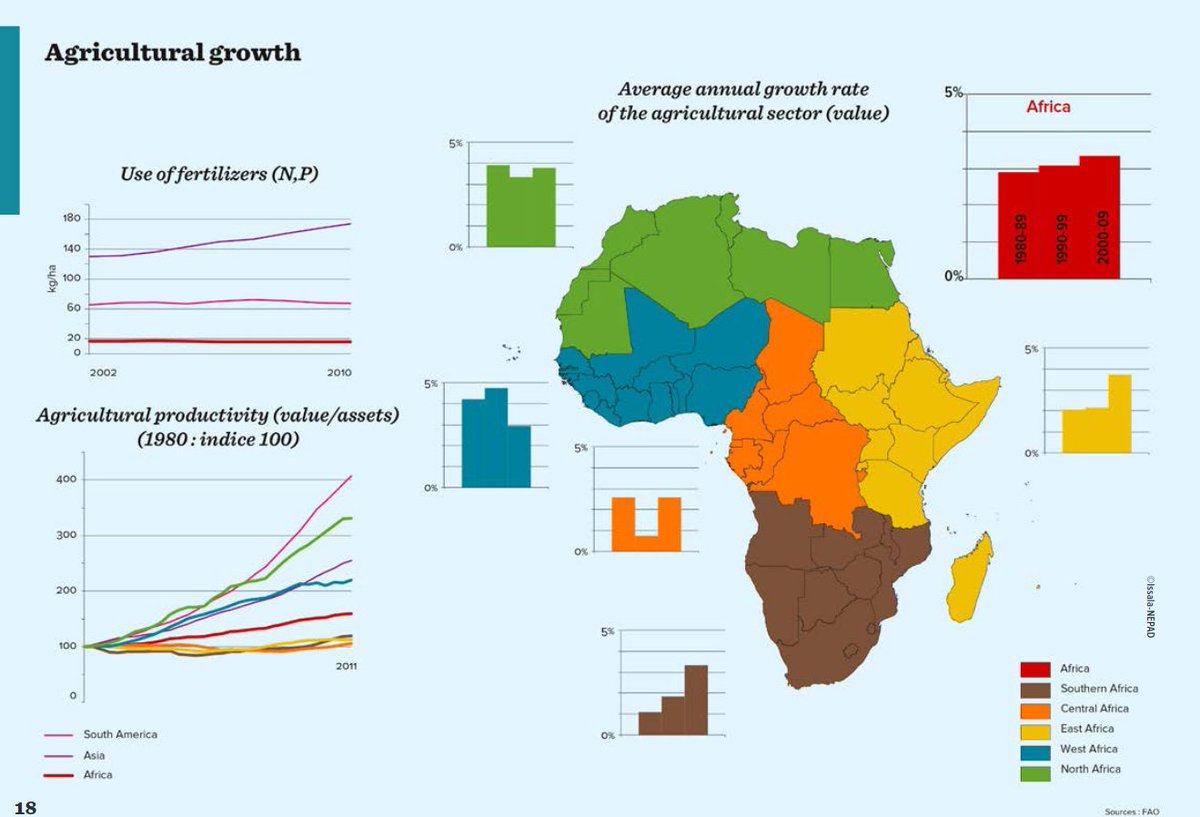
In Africa, agribusiness, more than any other sector, has the potential to reduce poverty and drive economic growth. Agriculture accounts for nearly half of the continent’s gross domestic product and employs 60 percent of the labor force.
#Cardano “Understanding Kamali”
#Cardano will be the underpinning of the emergence of Africa.
To grasp the full weight of the SOLUTIONS #Cardano can provide it is pertinent to read “Understanding Africa” as I will draw directly from the PROBLEMS laid out.
(2/50)
Here is a link if you have not already read
(1/38) #Cardano \u201cUnderstanding Africa\u201d (Part 1 of 2)
— FatCat (@fatcatofcrypto) February 10, 2021
This thread will be split into two parts with the 2nd coming out on Sunday.
Part 1 will layout the pervasive PROBLEMS Africa faces whereas Part 2 will apply direct technologies @InputOutputHK can implement as SOLUTIONS. pic.twitter.com/n3I91bnddq
(3/50)
What I will attempt to do here, is to create an immersive world for you to be placed in to grasp the weight and size of problems from the ground level and then take a grass-roots approach at solving them using #Cardano and its technology.
(4/50)
As an investor and community member of #Cardano, this should be extremely important to you as you have a stake (pun intended) in this.
“You are paid in direct proportion to the difficulty of the problems you solve” - @elonmusk
(5/50)
In Africa, agribusiness, more than any other sector, has the potential to reduce poverty and drive economic growth. Agriculture accounts for nearly half of the continent’s gross domestic product and employs 60 percent of the labor force.

You May Also Like



This is a pretty valiant attempt to defend the "Feminist Glaciology" article, which says conventional wisdom is wrong, and this is a solid piece of scholarship. I'll beg to differ, because I think Jeffery, here, is confusing scholarship with "saying things that seem right".
The article is, at heart, deeply weird, even essentialist. Here, for example, is the claim that proposing climate engineering is a "man" thing. Also a "man" thing: attempting to get distance from a topic, approaching it in a disinterested fashion.

Also a "man" thing—physical courage. (I guess, not quite: physical courage "co-constitutes" masculinist glaciology along with nationalism and colonialism.)

There's criticism of a New York Times article that talks about glaciology adventures, which makes a similar point.

At the heart of this chunk is the claim that glaciology excludes women because of a narrative of scientific objectivity and physical adventure. This is a strong claim! It's not enough to say, hey, sure, sounds good. Is it true?
Imagine for a moment the most obscurantist, jargon-filled, po-mo article the politically correct academy might produce. Pure SJW nonsense. Got it? Chances are you're imagining something like the infamous "Feminist Glaciology" article from a few years back.https://t.co/NRaWNREBvR pic.twitter.com/qtSFBYY80S
— Jeffrey Sachs (@JeffreyASachs) October 13, 2018
The article is, at heart, deeply weird, even essentialist. Here, for example, is the claim that proposing climate engineering is a "man" thing. Also a "man" thing: attempting to get distance from a topic, approaching it in a disinterested fashion.
Also a "man" thing—physical courage. (I guess, not quite: physical courage "co-constitutes" masculinist glaciology along with nationalism and colonialism.)
There's criticism of a New York Times article that talks about glaciology adventures, which makes a similar point.
At the heart of this chunk is the claim that glaciology excludes women because of a narrative of scientific objectivity and physical adventure. This is a strong claim! It's not enough to say, hey, sure, sounds good. Is it true?